

The impact of false positive COVID-19 results in an area of low prevalence
- PMID: 33243836
- PMCID: PMC7850182
- DOI: 10.7861/clinmed.2020-0839
The impact of false positive COVID-19 results in an area of low prevalence
Abstract
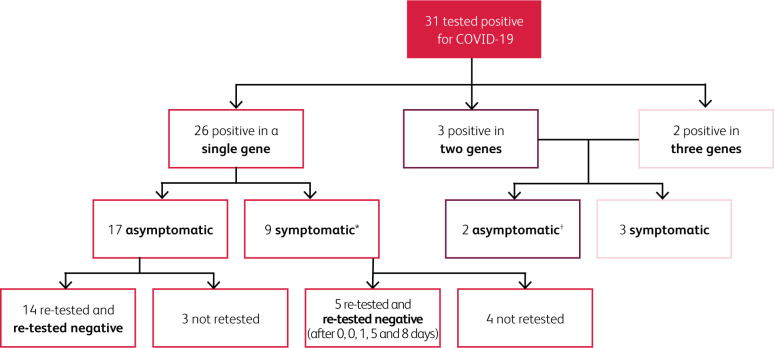
False negative results in COVID-19 testing are well recognised and frequently discussed. False positive results, while less common and less frequently discussed, still have several adverse implications, including potential exposure of a non-infected person to the virus in a cohorted area. Although false positive results are proportionally greater in low prevalence settings, the consequences are significant at all times and potentially of greater significance in high-prevalence settings. We evaluated COVID-19 results in one area during a period of low prevalence. The consequences of these results are discussed and implications for these results in both high and low prevalence settings are considered. We also provide recommendations to minimise the risk and impact of false-positive results.
Keywords: COVID-19; false positive results; high prevalence; low prevalence.
© Royal College of Physicians 2021. All rights reserved.
Figures
References
-
- Watson J, Whiting PF, Brush JE. Interpreting a Covid-19 test result. BMJ 2020;369:m1808. - PubMed
-
- Mayers C, Baker K. Impact of false-positives and false-negatives in the UK's COVID-19 RT-PCR testing programme. Government Office for Science, 2020. Available from www.gov.uk/government/publications/gos-impact-of-false-positives-and-neg... [Accessed 20 September 2020].
-
- Tenny S, Hoffman MR. Prevalence. StatPearls, 2020. Available from www.ncbi.nlm.nih.gov/books/NBK430867/ [Accessed 20 September 2020].
