

Identifying different phenotypes in takotsubo cardiomyopathy by latent class analysis
- PMID: 33244882
- PMCID: PMC7835582
- DOI: 10.1002/ehf2.13117
Identifying different phenotypes in takotsubo cardiomyopathy by latent class analysis
Abstract
Aims: This study sought to determine whether clinical clusters exist in takotsubo cardiomyopathy. Takotsubo cardiomyopathy (TCM) is a heterogeneous disorder with a complex, poorly understood pathogenesis. To better understand the heterogeneity of TCM, we identified different clinical phenotypes in a large sample of TCM patients by using latent class analysis (LCA).
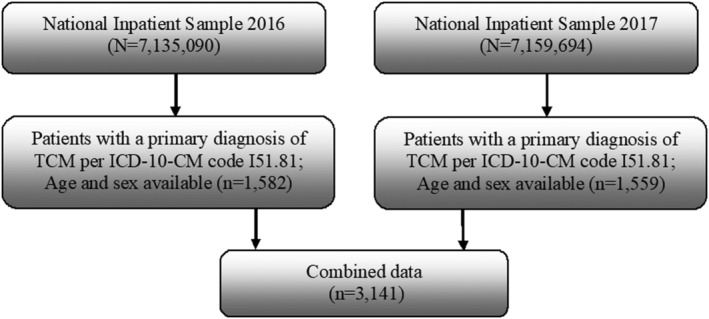
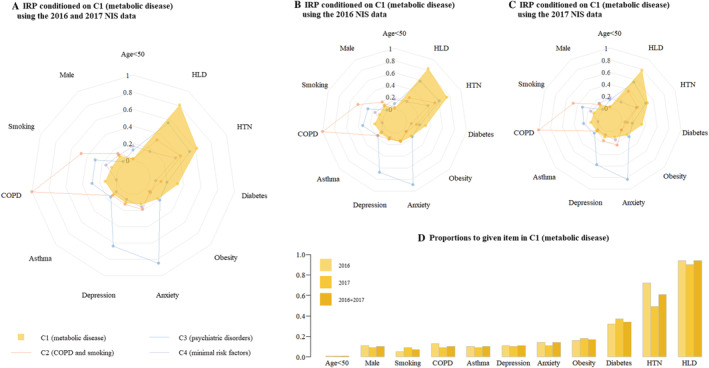
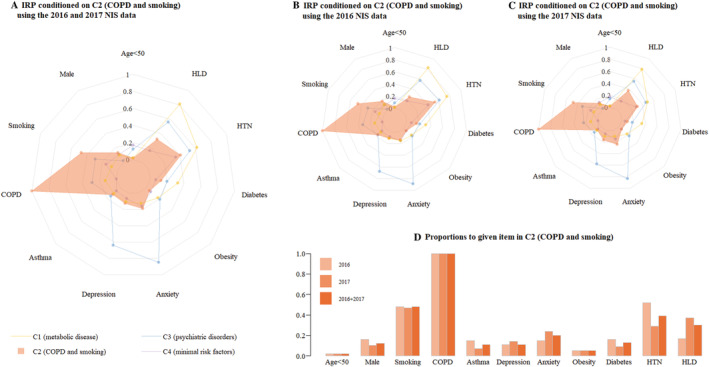
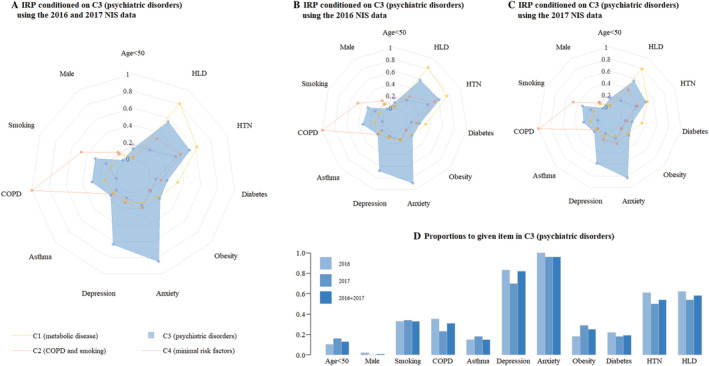
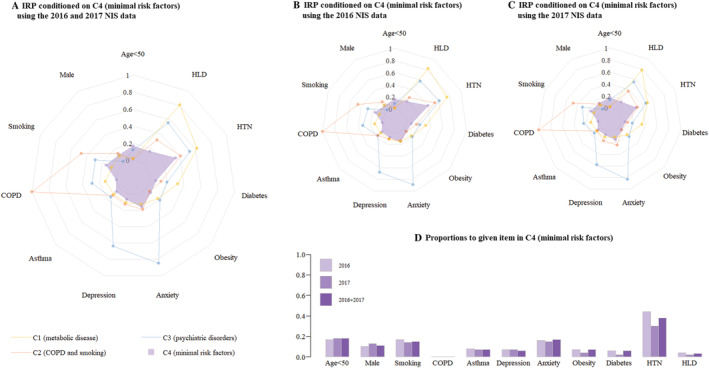
Methods and results: Using the National Inpatient Sample (NIS) database, we identified 3139 patients admitted to hospitals in 2016-2017 with a primary diagnosis of TCM. We performed LCA based on several patient demographics and comorbidities: age, sex, hypertension, hyperlipidaemia, diabetes mellitus, obesity, current smoking, asthma, chronic obstructive pulmonary disease (COPD), and anxiety and depressive disorders. We then repeated LCA separately with the NIS 2016 and 2017 data sets and performed a robust test to validate our results. We also compared in-hospital outcomes among the different clusters identified by LCA. Four patient clusters were identified. C1 (n = 1228, 39.4%) had the highest prevalence of hyperlipidaemia (93.4%), hypertension (61.6%), and diabetes (34.3%). In C2 (n = 440, 14.0%), all patients had COPD, and many were smokers (45.8%). C3 (n = 376, 11.8%) largely comprised patients with anxiety disorders (98.4%) and depressive disorders (80.1%). C4 (n = 1097, 34.8%) comprised patients with isolated TCM and few comorbidities. Among all clusters, C1 had the lowest in-hospital mortality (1.0%) and the shortest length of stay (3.2 ± 3.1 days), whereas C2 had the highest in-hospital mortality (3.4%).
Conclusions: Using LCA, we identified four clinical phenotypes of TCM. These may reflect different pathophysiological processes in TCM. Our findings may help identify treatment targets and select patients for future clinical trials.
Keywords: Latent class analysis; Phenotype; Takotsubo cardiomyopathy.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review. Eur Heart J 2006; 27: 1523–1529. - PubMed
-
- Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, Cammann VL, Sarcon A, Geyer V, Neumann CA, Seifert B, Hellermann J, Schwyzer M, Eisenhardt K, Jenewein J, Franke J, Katus HA, Burgdorf C, Schunkert H, Moeller C, Thiele H, Bauersachs J, Tschöpe C, Schultheiss HP, Laney CA, Rajan L, Michels G, Pfister R, Ukena C, Böhm M, Erbel R, Cuneo A, Kuck KH, Jacobshagen C, Hasenfuss G, Karakas M, Koenig W, Rottbauer W, Said SM, Braun‐Dullaeus RC, Cuculi F, Banning A, Fischer TA, Vasankari T, Airaksinen KEJ, Fijalkowski M, Rynkiewicz A, Pawlak M, Opolski G, Dworakowski R, MacCarthy P, Kaiser C, Osswald S, Galiuto L, Crea F, Dichtl W, Franz WM, Empen K, Felix SB, Delmas C, Lairez O, Erne P, Bax JJ, Ford I, Ruschitzka F, Prasad A, Lüscher TF. Clinical features and outcomes of takotsubo (stress) cardiomyopathy. N Engl J Med 2015; 373: 929–938. - PubMed
-
- Redfors B, Vedad R, Angerås O, Råmunddal T, Petursson P, Haraldsson I, Ali A, Dworeck C, Odenstedt J, Ioaness D, Libungan B, Shao Y, Albertsson P, Stone GW, Omerovic E. Mortality in takotsubo syndrome is similar to mortality in myocardial infarction—a report from the SWEDEHEART registry. Int J Cardiol 2015; 185: 282–289. - PubMed
-
- Naegele M, Flammer AJ, Enseleit F, Roas S, Frank M, Hirt A, Kaiser P, Cantatore S, Templin C, Fröhlich G, Romanens M, Lüscher TF, Ruschitzka F, Noll G, Sudano I. Endothelial function and sympathetic nervous system activity in patients with takotsubo syndrome. Int J Cardiol 2016; 224: 226–230. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
