

Diastolic dysfunction and mortality in 436 360 men and women: the National Echo Database Australia (NEDA)
- PMID: 33245344
- PMCID: PMC8081414
- DOI: 10.1093/ehjci/jeaa253
Diastolic dysfunction and mortality in 436 360 men and women: the National Echo Database Australia (NEDA)
Abstract
Aims: To examine the characteristics/prognostic impact of diastolic dysfunction (DD) according to 2016 American Society of Echocardiography (ASE) and European Society of Cardiovascular Imaging (ESCVI) guidelines, and individual parameters of DD.
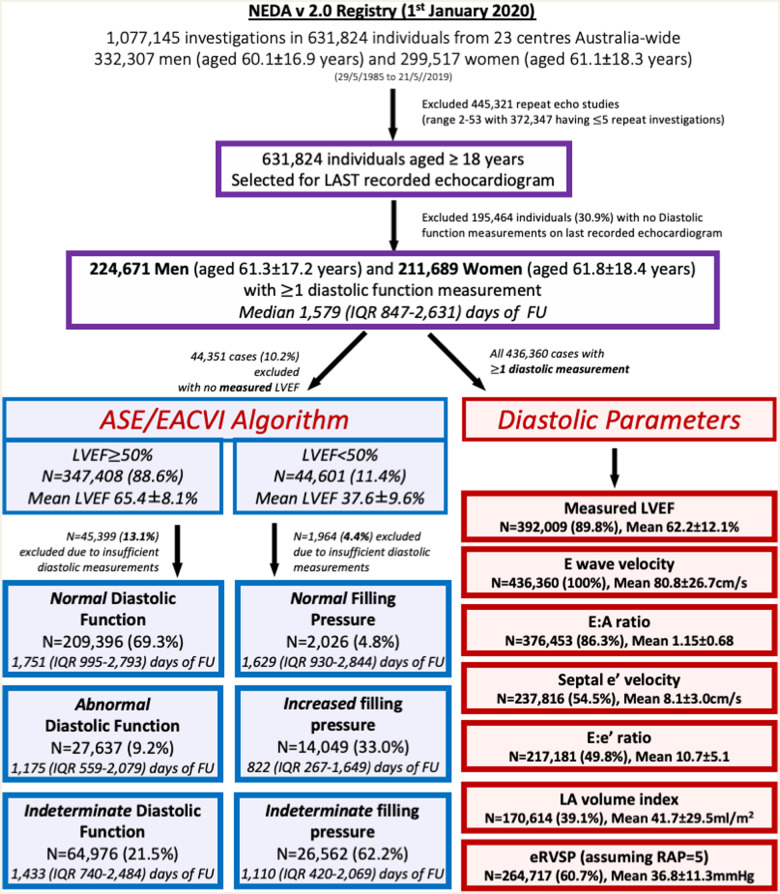
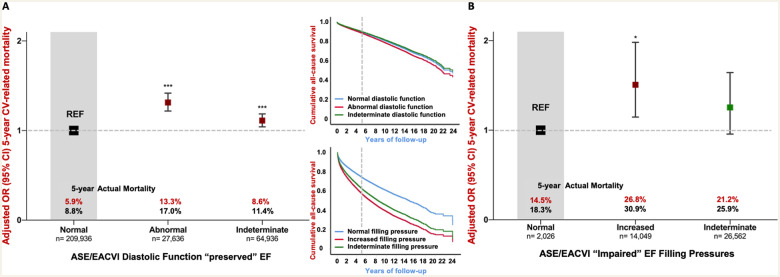
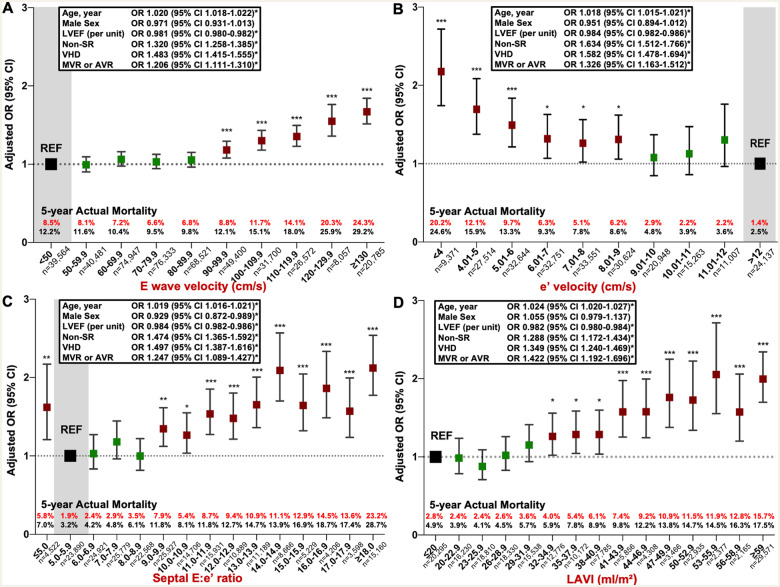
Methods and results: Data were derived from a large multicentre mortality-linked echocardiographic registry comprising 436 360 adults with ≥1 diastolic function measurement linked to 100 597 deaths during 2.2 million person-years follow-up. ASE/European Association of Cardiovascular Imaging (EACVI) algorithms could be applied in 392 009 (89.8%) cases; comprising 11.4% of cases with 'reduced' left ventricular ejection fraction (LVEF < 50%) and 88.6% with 'preserved' LVEF (≥50%). Diastolic function was indeterminate in 21.5% and 62.2% of 'preserved' and 'reduced' LVEF cases, respectively. Among preserved LVEF cases, the risk of adjusted 5-year cardiovascular-related mortality was elevated in both DD [odds ratio (OR) 1.31, 95% confidence interval (CI) 1.22-1.42; P < 0.001] and indeterminate status cases (OR 1.11, 95% CI 1.04-1.18; P < 0.001) vs. no DD. Among impaired LVEF cases, the equivalent risk of cardiovascular-related mortality was 1.51 (95% CI 1.15-1.98, P < 0.001) for increased filling pressure vs. 1.25 (95% CI 0.96-1.64, P = 0.06) for indeterminate status. Mitral E velocity, septal e' velocity, E:e' ratio, and LAVi all correlated with mortality. On adjusted basis, pivot-points of increased risk for cardiovascular-related mortality occurred at 90 cm/s for E wave velocity, 9 cm/s for septal e' velocity, an E:e' ratio of 9, and an LAVi of 32 mL/m2.
Conclusion: ASE/EACVI-classified DD is correlated with increased mortality. However, many cases remain 'indeterminate'. Importantly, when analysed individually, mitral E velocity, septal e' velocity, E:e' ratio, and LAVi revealed clear pivot-points of increased risk of cardiovascular-related mortality.
Keywords: big; data; diastolic; echocardiography; function; guidelines; mortality.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures

Comment in
-
Prognostic significance of left ventricular diastolic dysfunction and filling pressures based on current guideline recommendations.Eur Heart J Cardiovasc Imaging. 2021 Apr 28;22(5):516-517. doi: 10.1093/ehjci/jeaa254. Eur Heart J Cardiovasc Imaging. 2021. PMID: 33141914 No abstract available.
References
-
- Rossi A, Temporelli PL, Quintana M, Dini FL, Ghio S, Hillis GS. et al. ; on behalf of the MeRGE Heart Failure Collaborators. Independent relationship of left atrial size and mortality in patients with heart failure: an individual patient meta-analysis of longitudinal data (MeRGE Heart Failure). Eur J Heart Fail 2009;11:929–36. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM.. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006;355:251–9. - PubMed
-
- Møller JE, Whalley GA, Dini FL, Doughty RN, Gamble GD, Klein AL. et al. Independent prognostic importance of a restrictive left ventricular filling pattern after myocardial infarction: an individual patient meta-analysis: meta-Analysis Research Group in Echocardiography acute myocardial infarction. Circulation 2008;117:2591–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
