

Novel antisense therapy targeting microRNA-132 in patients with heart failure: results of a first-in-human Phase 1b randomized, double-blind, placebo-controlled study
- PMID: 33245749
- PMCID: PMC7954267
- DOI: 10.1093/eurheartj/ehaa898
Novel antisense therapy targeting microRNA-132 in patients with heart failure: results of a first-in-human Phase 1b randomized, double-blind, placebo-controlled study
Abstract
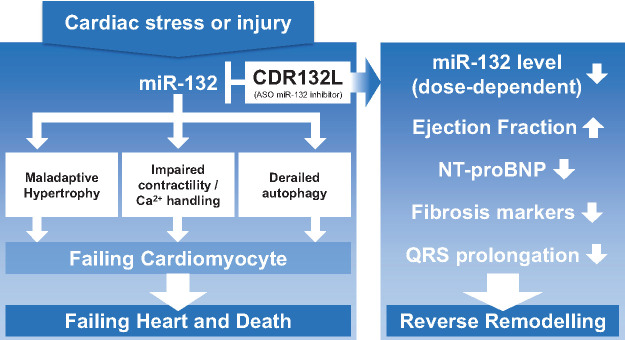
Aims: Cardiac microRNA-132-3p (miR-132) levels are increased in patients with heart failure (HF) and mechanistically drive cardiac remodelling processes. CDR132L, a specific antisense oligonucleotide, is a first-in-class miR-132 inhibitor that attenuates and even reverses HF in preclinical models. The aim of the current clinical Phase 1b study was to assess safety, pharmacokinetics, target engagement, and exploratory pharmacodynamic effects of CDR132L in patients on standard-of-care therapy for chronic ischaemic HF in a randomized, placebo-controlled, double-blind, dose-escalation study (NCT04045405).
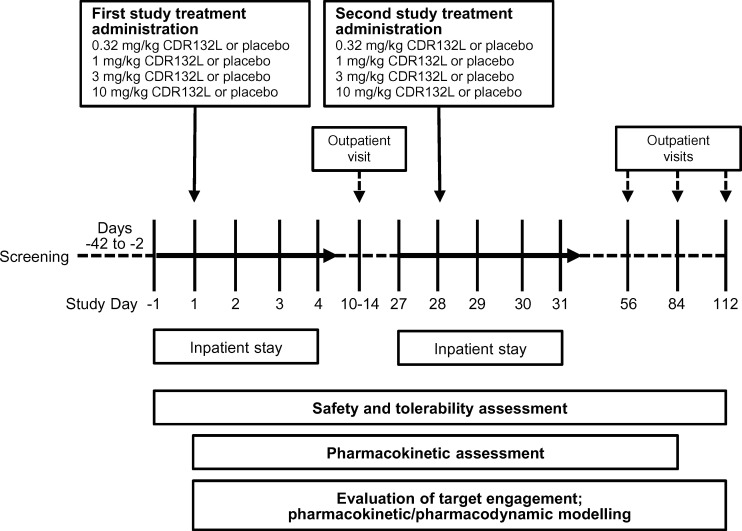
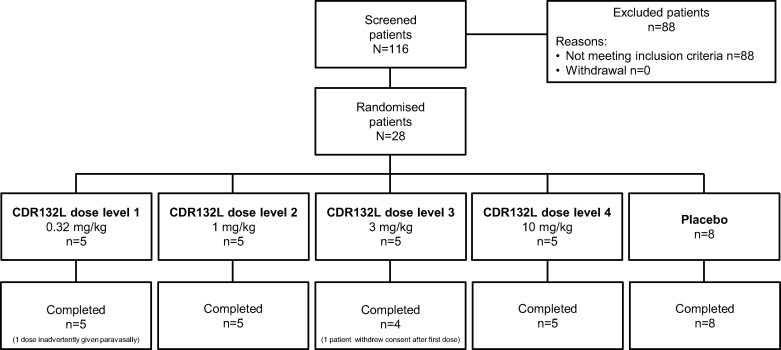
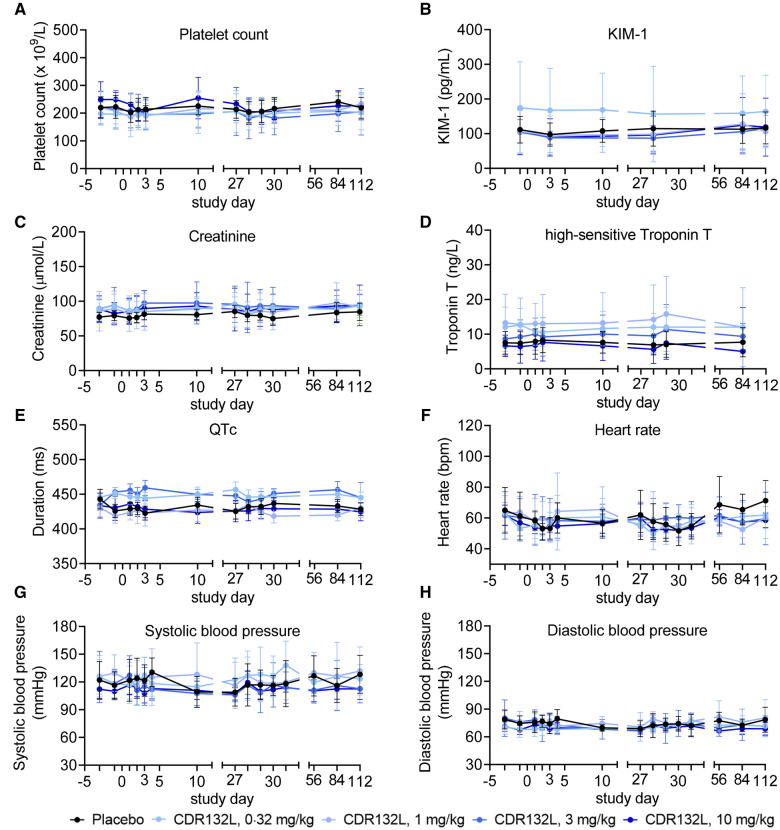
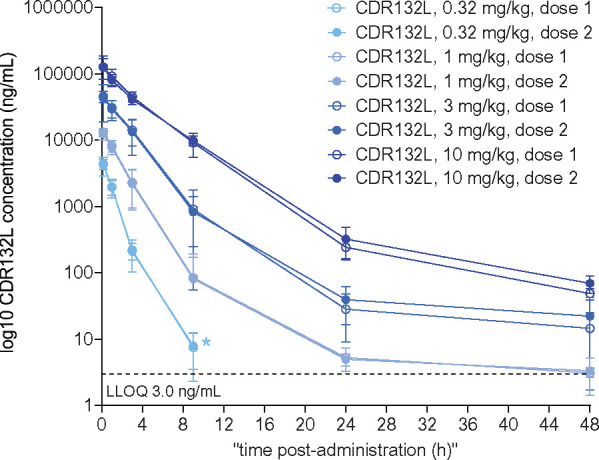
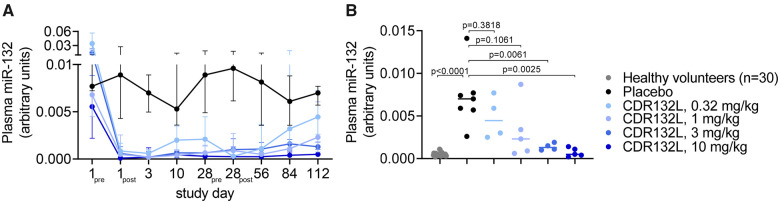
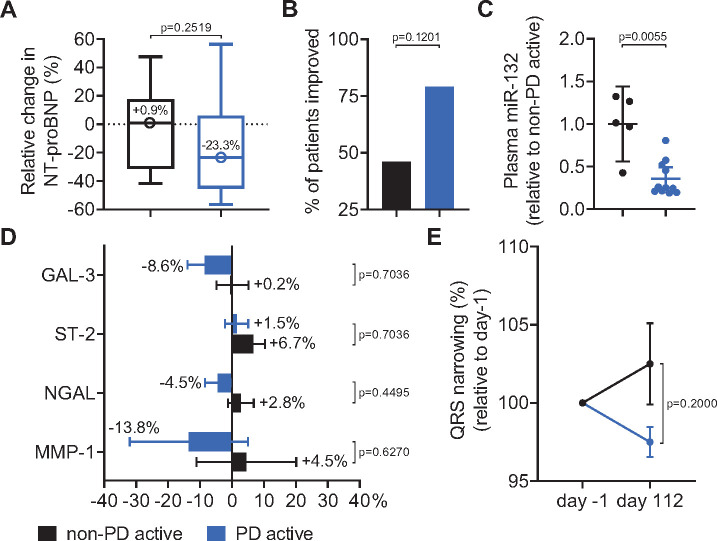
Methods and results: Patients had left ventricular ejection fraction between ≥30% and <50% or amino terminal fragment of pro-brain natriuretic peptide (NT-proBNP) >125 ng/L at screening. Twenty-eight patients were randomized to receive CDR132L (0.32, 1, 3, and 10 mg/kg body weight) or placebo (0.9% saline) in two intravenous infusions, 4 weeks apart in four cohorts of seven (five verum and two placebo) patients each. CDR132L was safe and well tolerated, without apparent dose-limiting toxicity. A pharmacokinetic/pharmacodynamic dose modelling approach suggested an effective dose level at ≥1 mg/kg CDR132L. CDR132L treatment resulted in a dose-dependent, sustained miR-132 reduction in plasma. Patients given CDR132L ≥1 mg/kg displayed a median 23.3% NT-proBNP reduction, vs. a 0.9% median increase in the control group. CDR132L treatment induced significant QRS narrowing and encouraging positive trends for relevant cardiac fibrosis biomarkers.
Conclusion: This study is the first clinical trial of an antisense drug in HF patients. CDR132L was safe and well tolerated, confirmed linear plasma pharmacokinetics with no signs of accumulation, and suggests cardiac functional improvements. Although this study is limited by the small patient numbers, the indicative efficacy of this drug is very encouraging justifying additional clinical studies to confirm the beneficial CDR132L pharmacodynamic effects for the treatment of HF.
Keywords: Cardiac remodelling; Clinical trial Phase 1b study; Heart failure; microRNAs.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Antagonism of miRNA in heart failure: first evidence in human.Eur Heart J. 2021 Jan 7;42(2):189-191. doi: 10.1093/eurheartj/ehaa967. Eur Heart J. 2021. PMID: 33338200 Free PMC article. No abstract available.
References
-
- Braunwald E. The war against heart failure: the Lancet lecture. Lancet 2015;385:812–824. - PubMed
-
- Rossignol P, Hernandez AF, Solomon SD, Zannad F.. Heart failure drug treatment. Lancet 2019;393:1034–1044. - PubMed
-
- Ucar A, Gupta SK, Fiedler J, Erikci E, Kardasinski M, Batkai S, Dangwal S, Kumarswamy R, Bang C, Holzmann A, Remke J, Caprio M, Jentzsch C, Engelhardt S, Geisendorf S, Glas C, Hofmann TG, Nessling M, Richter K, Schiffer M, Carrier L, Napp LC, Bauersachs J, Chowdhury K, Thum T.. The miRNA-212/132 family regulates both cardiac hypertrophy and cardiomyocyte autophagy. Nat Commun 2012;3:1078. - PMC - PubMed
-
- Foinquinos A, Batkai S, Genschel C, Viereck J, Rump S, Gyöngyösi M, Traxler D, Riesenhuber M, Spannbauer A, Lukovic D, Weber N, Zlabinger K, Hašimbegović E, Winkler J, Fiedler J, Dangwal S, Fischer M, Roche J. D L, Wojciechowski D, Kraft T, Garamvölgyi R, Neitzel S, Chatterjee S, Yin X, Bär C, Mayr M, Xiao K, Thum T.. Preclinical development of a miR-132 inhibitor for heart failure treatment. Nat Commun 2020;11:633. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
