

doi: 10.1038/s41375-020-01093-1.
Epub 2020 Nov 27.
STAT3 and TP53 mutations associate with poor prognosis in anaplastic large cell lymphoma
Affiliations
- PMID: 33247178
- PMCID: PMC8102183
- DOI: 10.1038/s41375-020-01093-1
Item in Clipboard
STAT3 and TP53 mutations associate with poor prognosis in anaplastic large cell lymphoma
Leukemia.
2021 May.
No abstract available
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
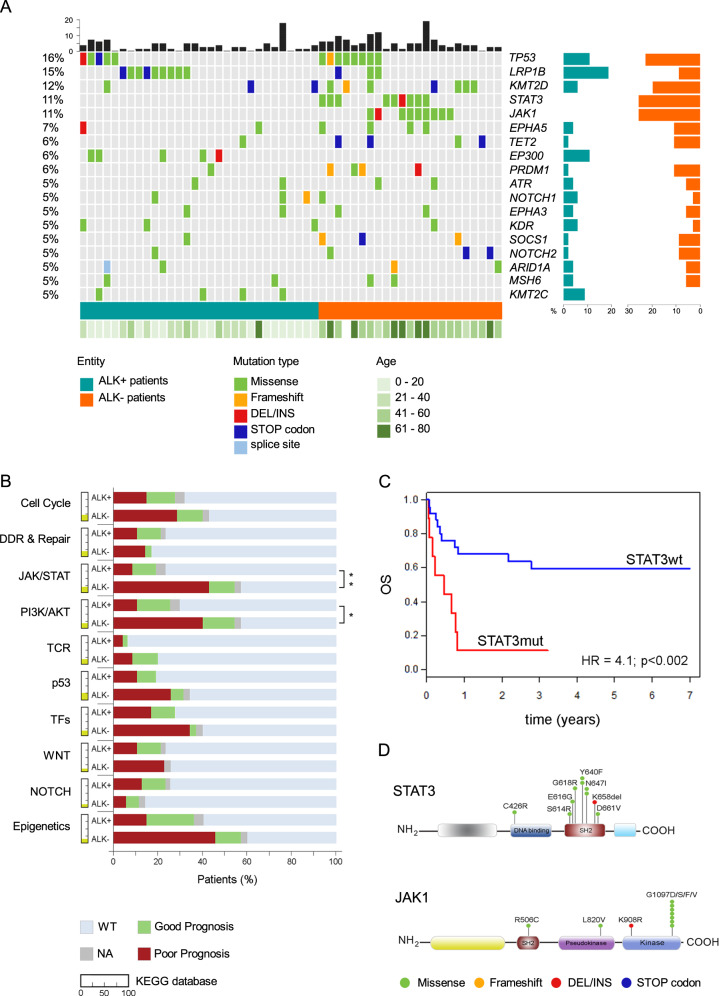
a Oncoplot shows the genes mutated in at least 5% of the entire cohort. The percentage is shown on the left axis. Each column represents a patient, ALK+ in dark green and ALK− ALCL patients in dark orange. The black bars on the top represent the number of mutated genes in each patient. On the right axis, the frequency of mutated gene in ALK+ (dark green) and ALK− (dark orange) ALCL patients. The green bar on the bottom shows the age of each patient. Mutation types are represented in different colors as shown in the legend. b Percentage of patients harboring at least one mutated gene in ten biological pathways. The yellow colored portion next to each pathway indicates the percentage of genes present in our panel that belong to that specific pathway according to the KEGG database. For each pathway shown, the patients are divided according to prognosis; red: patients with poor prognosis; green: patients with good prognosis; gray: patients for whom clinical information is not available (NA); light blue patients wildtype (WT) that do not harbor mutated genes in that specific pathway. The patients are represented as percentage of the total. DDR and repair DNA damage response and repair pathway, TFs transcription factors. Fisher’s exact test: *p < 0.05, **p < 0.01 and ***p < 0.001. c 7-year OS of ALK− ALCL patients according to STAT3 status: STAT3 mutated (red) versus STAT3 wt (blue). P values and hazard ratios (HR) shown were determined by the Cox proportional hazards model. d Schematic representation of STAT3 and JAK1 domains and the position of the variants.
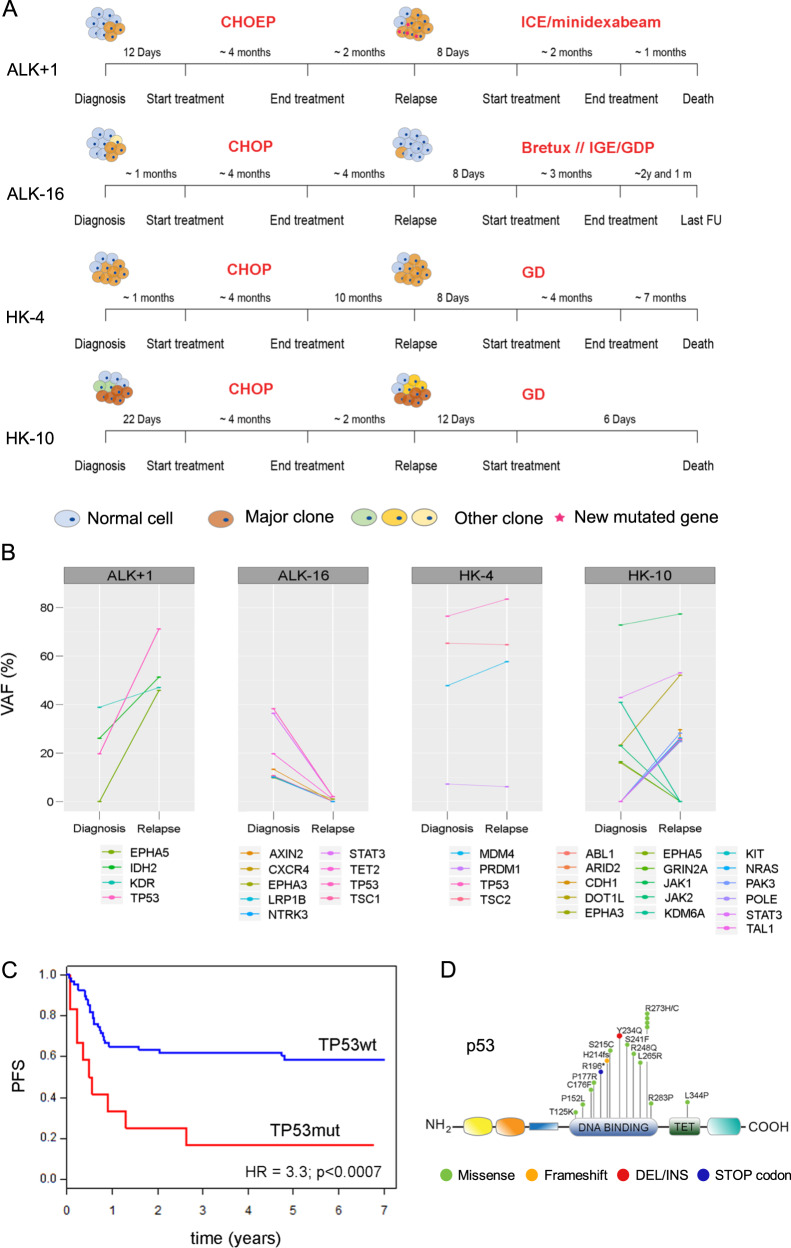
a Schematic representation of four patients sequenced at diagnosis and at relapse highlighting their clinical path and treatment. Meaning of the color is described in the legend. CHOEP chemotherapy with cyclophosphamide, doxorubicin, etoposide, vincristine and prednisone, CHOP chemotherapy with cyclophosphamide, doxorubicin, vincristine and prednisone, ICE chemotherapy combination that includes ifosfamide, carboplatin and etoposide, bretux: brentuximab vedotin, GDP gemcitabine, dexamethasone, and cisplatin, GD gemcitabine and docetaxel, FU follow up. b Changes in mutational burden during tumor progression. The percentage of variant allele frequency (VAF%) for each gene is plotted at diagnosis and at relapse. The names of genes involved are reported under each plot. c 7-year PFS in systemic ALCL patients according to TP53 status; red: TP53 mutated (mut) patients; blue: TP53 wild-type (wt) patients. P values and hazard ratios (HR) shown were determined by Cox proportional hazards. d Schematic representation of p53 domains and the variants detected.
References
-
- Savage KJ, Harris NL, Vose JM, Ullrich F, Jaffe ES, Connors JM, et al. ALK- anaplastic large-cell lymphoma is clinically and immunophenotypically different from both ALK+ ALCL and peripheral T-cell lymphoma, not otherwise specified: report from the International Peripheral T-Cell Lymphoma Project. Blood. 2008;111:5496–504. doi: 10.1182/blood-2008-01-134270. - DOI - PubMed
-
- Janikova A, Chloupkova R, Campr V, Klener P, Hamouzova J, Belada D, et al. First-line therapy for T cell lymphomas: a retrospective population-based analysis of 906 T cell lymphoma patients. Ann Hematol. 2019. http://link.springer.com/10.1007/s00277-019-03694-y. - DOI - PubMed
-
- Hapgood G, Savage KJ. The biology and management of systemic anaplastic large cell lymphoma. Blood. 2015;2:17–25. https://pubmed.ncbi.nlm.nih.gov/25869285/. - PubMed
-
- Brugières L, Deley MC Le, Pacquement H, Meguerian-Bedoyan Z, Terrier-Lacombe MJ, Robert A, et al. CD30+ anaplastic large-cell lymphoma in children: analysis of 82 patients enrolled in two consecutive studies of the French Society of Pediatric Oncology. Blood. 1998;92:3591–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
