

Neuromuscular Function of the Knee Joint Following Knee Injuries: Does It Ever Get Back to Normal? A Systematic Review with Meta-Analyses
- PMID: 33247378
- PMCID: PMC7846527
- DOI: 10.1007/s40279-020-01386-6
Neuromuscular Function of the Knee Joint Following Knee Injuries: Does It Ever Get Back to Normal? A Systematic Review with Meta-Analyses
Abstract
Background: Neuromuscular deficits are common following knee injuries and may contribute to early-onset post-traumatic osteoarthritis, likely mediated through quadriceps dysfunction.
Objective: To identify how peri-articular neuromuscular function changes over time after knee injury and surgery.
Design: Systematic review with meta-analyses.
Data sources: PubMed, Web of Science, Embase, Scopus, CENTRAL (Trials).
Eligibility criteria for selecting studies: Moderate and high-quality studies comparing neuromuscular function of muscles crossing the knee joint between a knee-injured population (ligamentous, meniscal, osteochondral lesions) and healthy controls. Outcomes included normalized isokinetic strength, muscle size, voluntary activation, cortical and spinal-reflex excitability, and other torque related outcomes.
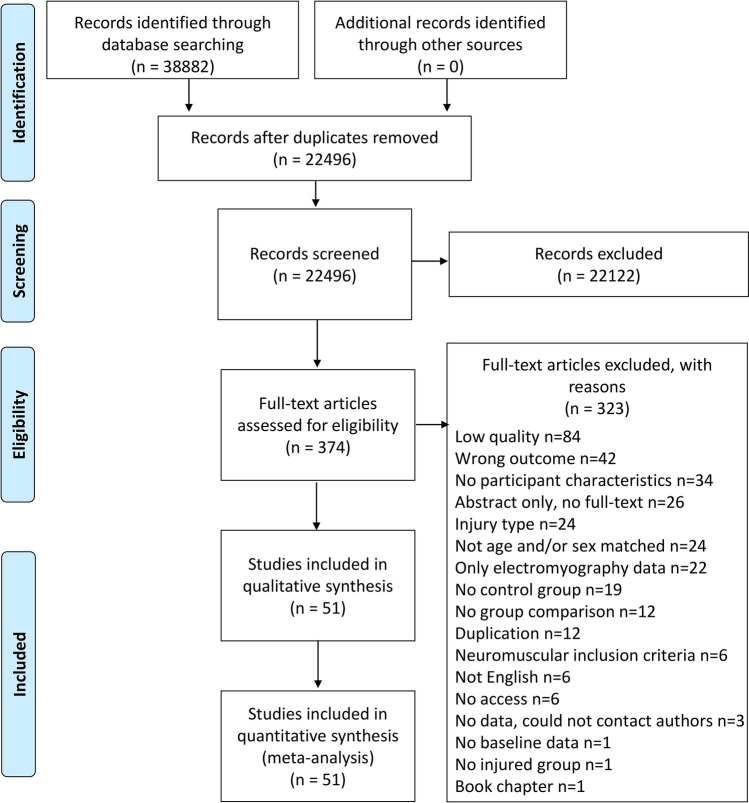
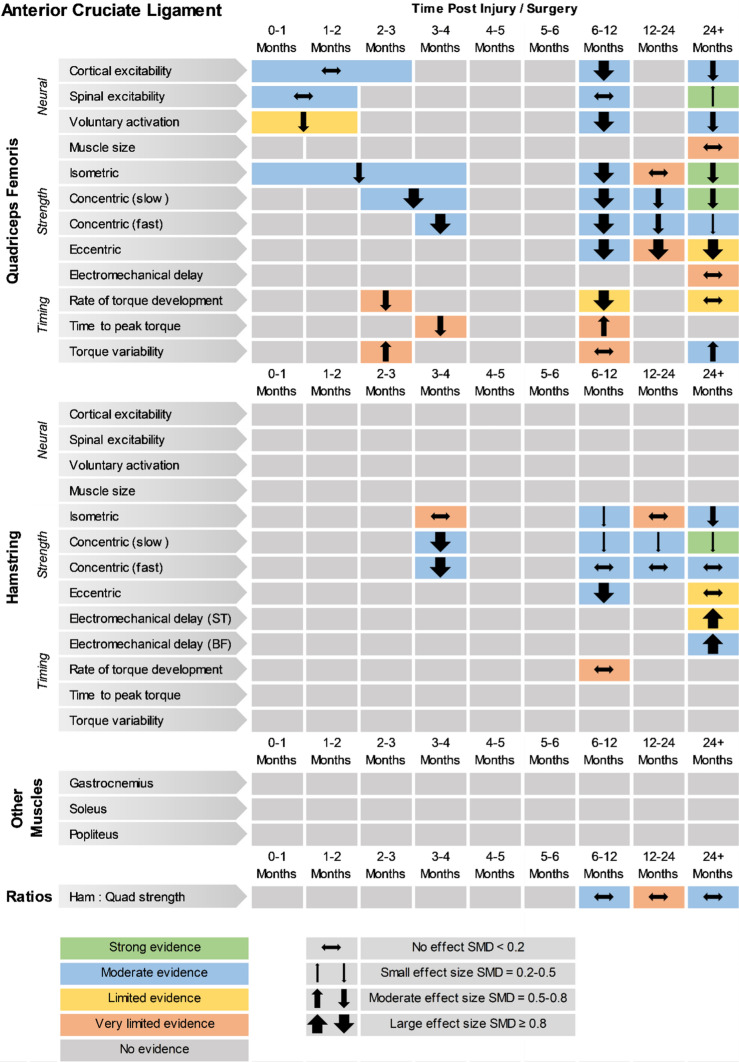
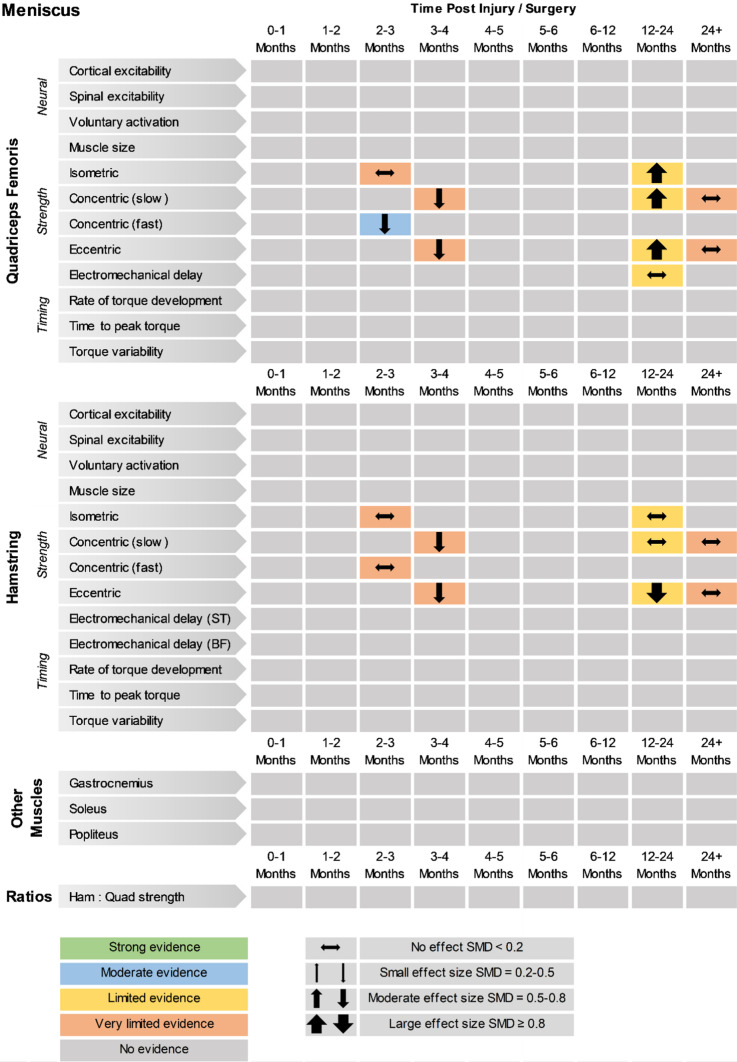
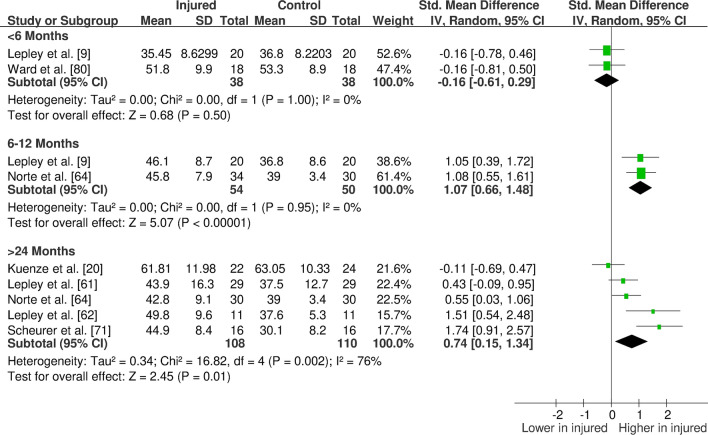
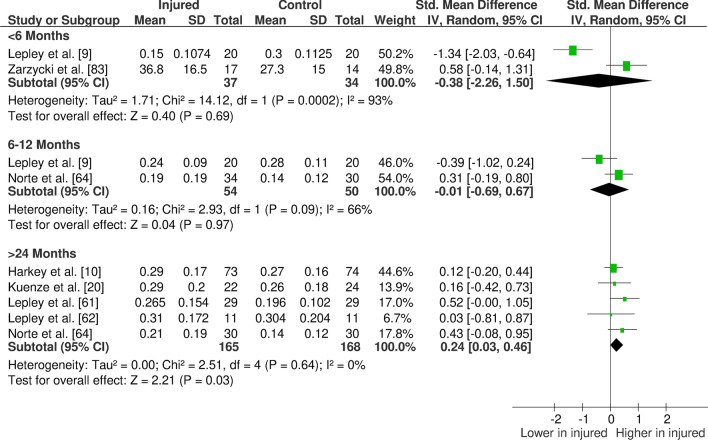
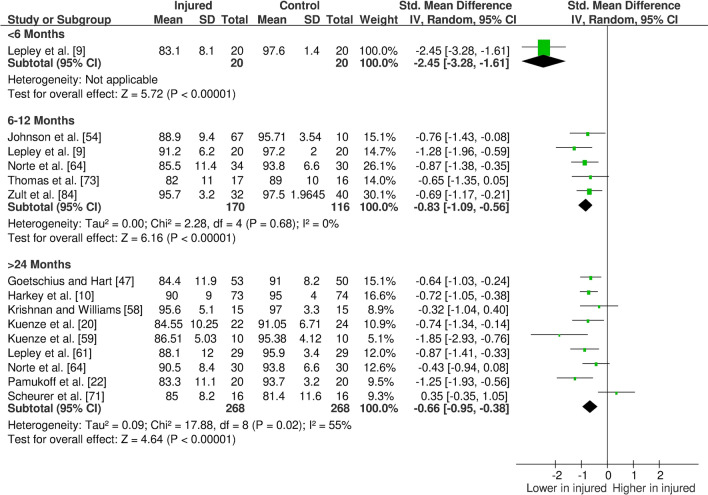
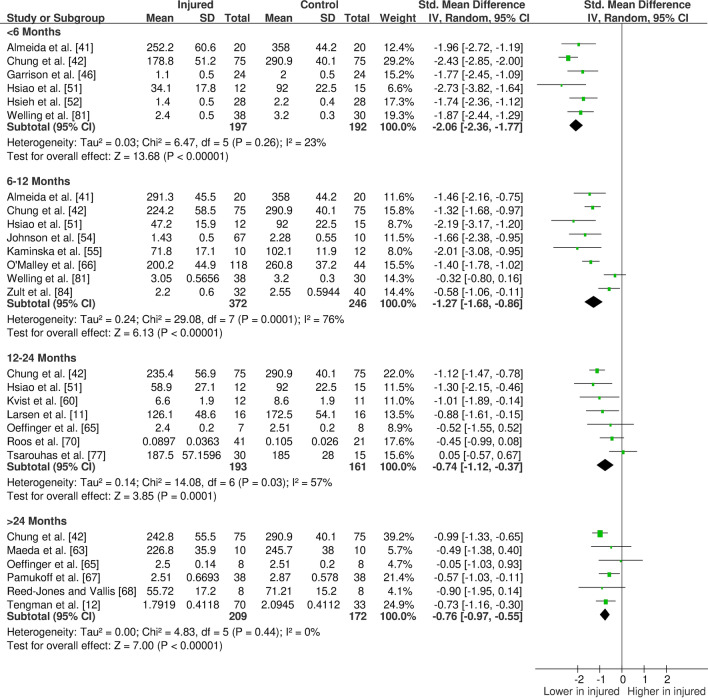
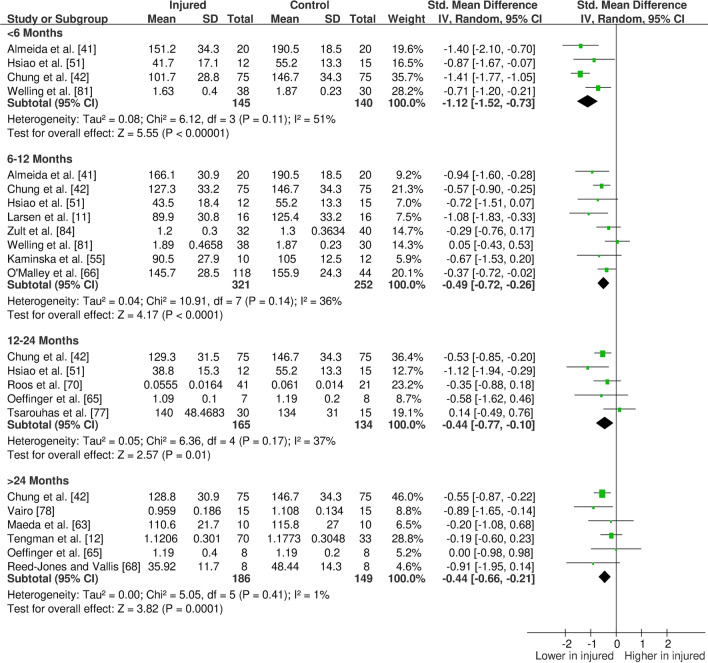
Results: A total of 46 studies of anterior cruciate ligament (ACL) and five of meniscal injury were included. For ACL injury, strength and voluntary activation deficits were evident (moderate to strong evidence). Cortical excitability was not affected at < 6 months (moderate evidence) but decreased at 24+ months (moderate evidence). Spinal-reflex excitability did not change at < 6 months (moderate evidence) but increased at 24+ months (strong evidence). We also found deficits in torque variability, rate of torque development, and electromechanical delay (very limited to moderate evidence). For meniscus injury, strength deficits were evident only in the short-term. No studies reported gastrocnemius, soleus or popliteus muscle outcomes for either injury. No studies were found for other ligamentous or chondral injuries.
Conclusions: Neuromuscular deficits persist for years post-injury/surgery, though the majority of evidence is from ACL injured populations. Muscle strength deficits are accompanied by neural alterations and changes in control and timing of muscle force, but more studies are needed to fill the evidence gaps we have identified. Better characterisation and therapeutic strategies addressing these deficits could improve rehabilitation outcomes, and potentially prevent PTOA.
Trial registration number: PROSPERO CRD42019141850.
Conflict of interest statement
Beyza Tayfur, Chedsada Charuphongsa, Dylan Morrissey and Stuart Miller declare that they have no conflicts of interest relevant to the content of this review.
Figures
References
-
- Muthuri SG, McWilliams DF, Doherty M, Zhang W. History of knee injuries and knee osteoarthritis: a meta-analysis of observational studies. Osteoarthr Cartil. 2011;19:1286–1293. - PubMed
-
- Poulsen E, Goncalves GH, Bricca A, Roos EM, Thorlund JB, Juhl CB. Knee osteoarthritis risk is increased 4–6 fold after knee injury - a systematic review and meta-analysis. Br J Sports Med. 2019;53:1454–1463. - PubMed
-
- Snoeker B, Turkiewicz A, Magnusson K, Frobell R, Yu D, Peat G, et al. Risk of knee osteoarthritis after different types of knee injuries in young adults: a population-based cohort study. Br J Sport Med. 2020;54:725–730. - PubMed
-
- Lie MM, Risberg MA, Storheim K, Engebretsen L, Øiestad BE. What’s the rate of knee osteoarthritis 10 years after anterior cruciate ligament injury? An updated systematic review. Br J Sports Med. 2019;53:1162–1167. - PubMed
-
- Carbone A, Rodeo S. Review of current understanding of post-traumatic osteoarthritis resulting from sports injuries. J Orthop Res. 2017;35:397–405. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
