

RAMIE: tradition drives innovation-feasibility of a robotic-assisted intra-thoracic anastomosis
- PMID: 33247384
- PMCID: PMC7694887
- DOI: 10.1007/s13304-020-00932-1
RAMIE: tradition drives innovation-feasibility of a robotic-assisted intra-thoracic anastomosis
Abstract
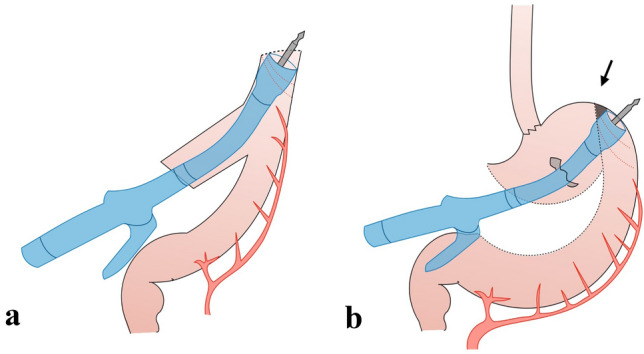
Due to the difficulties in the intra-thoracic esophagogastric anastomosis creation, totally minimally invasive Ivor Lewis esophagectomy (MIE) did not encountered a large diffusion, preferring hybrid techniques or cervical anastomosis. Robot-assisted minimally invasive esophagectomy (RAMIE) has gained popularity due to an easy reproducibility of the open anastomotic technique. In this feasibility study, we described the RAMIE technique introduced in our Center, providing innovative details for a mechanical end-to-end anastomosis. With patient in prone position, esophagectomy is conducted through the meso-esophagus plan. Robotic hand-sewn purse-string is realized above Azygos vein. A 4-cm thoracotomy in the fifth intercostal space is performed by enlarging the trocar incision. The tubulization is performed to create an access pouch for the introduction of the circular stapler. After the creation of the end-to-end anastomosis, the access pouch is resected and a robotic over-sewn is realized. From January 2020 until July 2020, ten patients were enrolled. No restriction in term of age, BMI, ASA grade or previous surgery were applied. Median operative time was 700 min. R0 resection was achieved in all cases with a good lymph node harvesting. No anastomotic leak or stricture were observed. One chyle leak was treated conservatively. Median length of stay was 8 days and 90 days mortality was 0%. This study evidenced how robotic surgery allowed us to perform the same anastomosis of our open technique with good oncological results and morbidity and length of stay comparable with our previous results. Of note, longer operative time has been recorded. Further studies after the completion of the learning curve are necessary to address more definite conclusions.
Keywords: Ivor lewis; RAMIE; Robotic surgery.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
-
- Straatman J, van der Wielen N, Nieuwenhuijzen GA, et al. Techniques and short-term outcomes for total minimally invasive Ivor Lewis esophageal resection in distal esophageal and gastroesophageal junction cancers: pooled data from six European centers. Surg Endosc. 2017;31(1):119–126. doi: 10.1007/s00464-016-4938-2. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
