

The clinically used serine protease inhibitor nafamostat reduces influenza virus replication and cytokine production in human airway epithelial cells and viral replication in mice
- PMID: 33247612
- PMCID: PMC7753675
- DOI: 10.1002/jmv.26700
The clinically used serine protease inhibitor nafamostat reduces influenza virus replication and cytokine production in human airway epithelial cells and viral replication in mice
Abstract
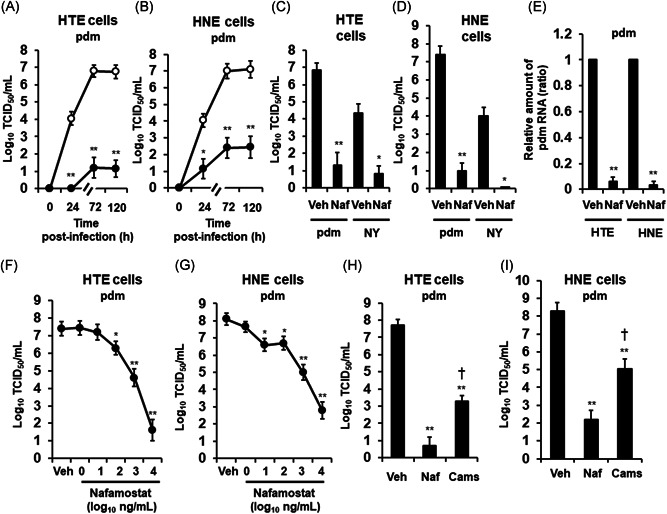
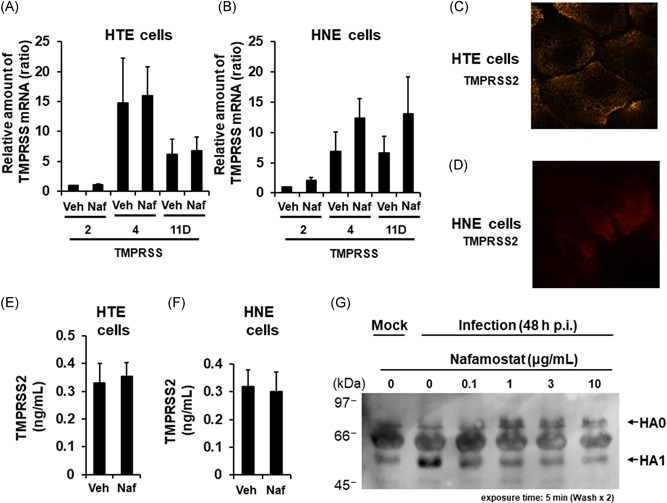
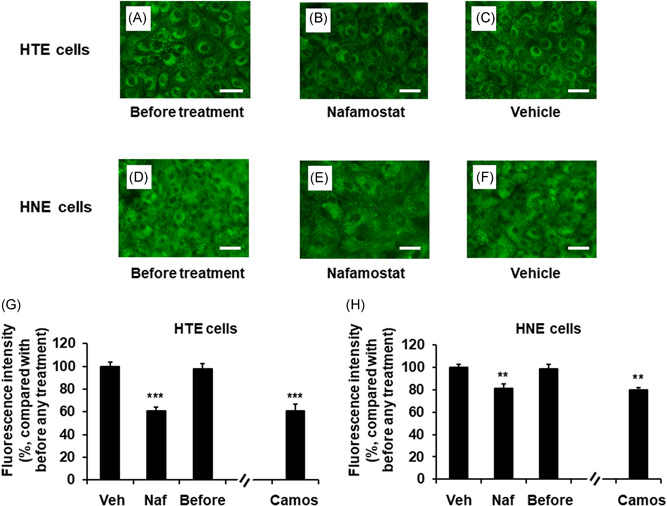
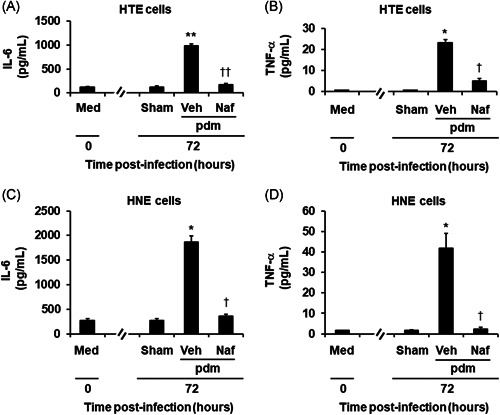
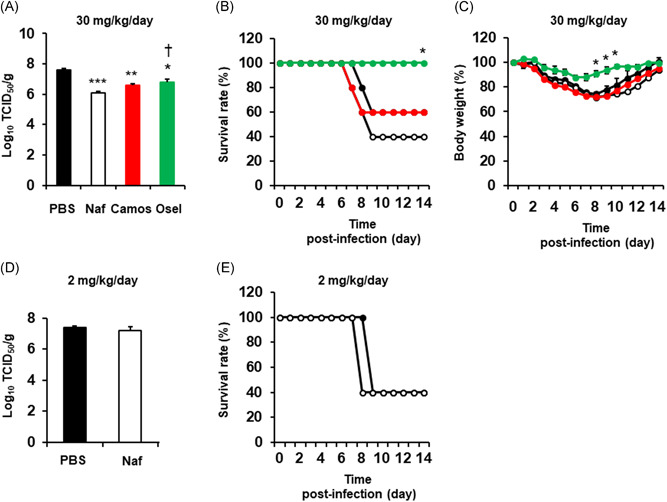
The effects of the clinically used protease inhibitor nafamostat on influenza virus replication have not been well studied. Primary human tracheal (HTE) and nasal (HNE) epithelial cells were pretreated with nafamostat and infected with the 2009 pandemic [A/Sendai-H/108/2009/(H1N1) pdm09] or seasonal [A/New York/55/2004(H3N2)] influenza virus. Pretreatment with nafamostat reduced the titers of the pandemic and seasonal influenza viruses and the secretion of inflammatory cytokines, including interleukin-6 and tumor necrosis factor-α, in the supernatants of the cells infected with the pandemic influenza virus. HTE and HNE cells exhibited mRNA and/or protein expression of transmembrane protease serine 2 (TMPRSS2), TMPRSS4, and TMPRSS11D. Pretreatment with nafamostat reduced cleavage of the precursor protein HA0 of the pandemic influenza virus into subunit HA1 in HTE cells and reduced the number of acidic endosomes in HTE and HNE cells where influenza virus RNA enters the cytoplasm. Additionally, nafamostat (30 mg/kg/day, intraperitoneal administration) reduced the levels of the pandemic influenza virus [A/Hyogo/YS/2011 (H1N1) pdm09] in mouse lung washes. These findings suggest that nafamostat may inhibit influenza virus replication in human airway epithelial cells and mouse lungs and reduce infection-induced airway inflammation by modulating cytokine production.
Keywords: antiviral agents; cell cultures; cytokines; influenza virus; protease inhibitor; respiratory tract.
© 2020 Wiley Periodicals LLC.
Figures
Similar articles
-
The TMPRSS2 Inhibitor Nafamostat Reduces SARS-CoV-2 Pulmonary Infection in Mouse Models of COVID-19.mBio. 2021 Aug 31;12(4):e0097021. doi: 10.1128/mBio.00970-21. Epub 2021 Aug 3. mBio. 2021. PMID: 34340553 Free PMC article.
-
The serine protease inhibitor camostat inhibits influenza virus replication and cytokine production in primary cultures of human tracheal epithelial cells.Pulm Pharmacol Ther. 2015 Aug;33:66-74. doi: 10.1016/j.pupt.2015.07.001. Epub 2015 Jul 10. Pulm Pharmacol Ther. 2015. PMID: 26166259 Free PMC article.
-
Nafamostat reduces systemic inflammation in TLR7-mediated virus-like illness.J Neuroinflammation. 2022 Jan 6;19(1):8. doi: 10.1186/s12974-021-02357-y. J Neuroinflammation. 2022. PMID: 34991643 Free PMC article.
-
TMPRSS2 inhibitors for the treatment of COVID-19 in adults: a systematic review and meta-analysis of randomized clinical trials of nafamostat and camostat mesylate.Clin Microbiol Infect. 2024 Jun;30(6):743-754. doi: 10.1016/j.cmi.2024.01.029. Epub 2024 Feb 6. Clin Microbiol Infect. 2024. PMID: 38331253
-
Airway proteases: an emerging drug target for influenza and other respiratory virus infections.Curr Opin Virol. 2017 Jun;24:16-24. doi: 10.1016/j.coviro.2017.03.018. Epub 2017 Apr 14. Curr Opin Virol. 2017. PMID: 28414992 Free PMC article. Review.
Cited by
-
Potent sialic acid inhibitors that target influenza A virus hemagglutinin.Sci Rep. 2021 Apr 21;11(1):8637. doi: 10.1038/s41598-021-87845-0. Sci Rep. 2021. PMID: 33883588 Free PMC article.
-
The TMPRSS2 Inhibitor Nafamostat Reduces SARS-CoV-2 Pulmonary Infection in Mouse Models of COVID-19.mBio. 2021 Aug 31;12(4):e0097021. doi: 10.1128/mBio.00970-21. Epub 2021 Aug 3. mBio. 2021. PMID: 34340553 Free PMC article.
-
Co-administration of Favipiravir and the Remdesivir Metabolite GS-441524 Effectively Reduces SARS-CoV-2 Replication in the Lungs of the Syrian Hamster Model.mBio. 2021 Feb 22;13(1):e0304421. doi: 10.1128/mbio.03044-21. Epub 2022 Feb 1. mBio. 2021. PMID: 35100870 Free PMC article.
-
Multicenter, single-blind, randomized controlled study of the efficacy and safety of favipiravir and nafamostat mesilate in patients with COVID-19 pneumonia.Int J Infect Dis. 2023 Mar;128:355-363. doi: 10.1016/j.ijid.2022.12.039. Epub 2023 Jan 4. Int J Infect Dis. 2023. PMID: 36610659 Free PMC article. Clinical Trial.
-
TMPRSS2 Activates Hemagglutinin-Esterase Glycoprotein of Influenza C Virus.J Virol. 2021 Oct 13;95(21):e0129621. doi: 10.1128/JVI.01296-21. Epub 2021 Aug 18. J Virol. 2021. PMID: 34406864 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
