

Cardiac resynchronization therapy and its effects in patients with type 2 DIAbetes mellitus OPTimized in automatic vs. echo guided approach. Data from the DIA-OPTA investigators
- PMID: 33248462
- PMCID: PMC7700711
- DOI: 10.1186/s12933-020-01180-8
Cardiac resynchronization therapy and its effects in patients with type 2 DIAbetes mellitus OPTimized in automatic vs. echo guided approach. Data from the DIA-OPTA investigators
Abstract
Objectives: To evaluate the effects of cardiac resynchronization therapy (CRTd) in patients with type 2 diabetes mellitus (T2DM) optimized via automatic vs. echocardiography-guided approach.
Background: The suboptimal atrio-ventricular (AV) and inter-ventricular (VV) delays optimization reduces CRTd response. Therefore, we hypothesized that automatic CRTd optimization might improve clinical outcomes in T2DM patients.
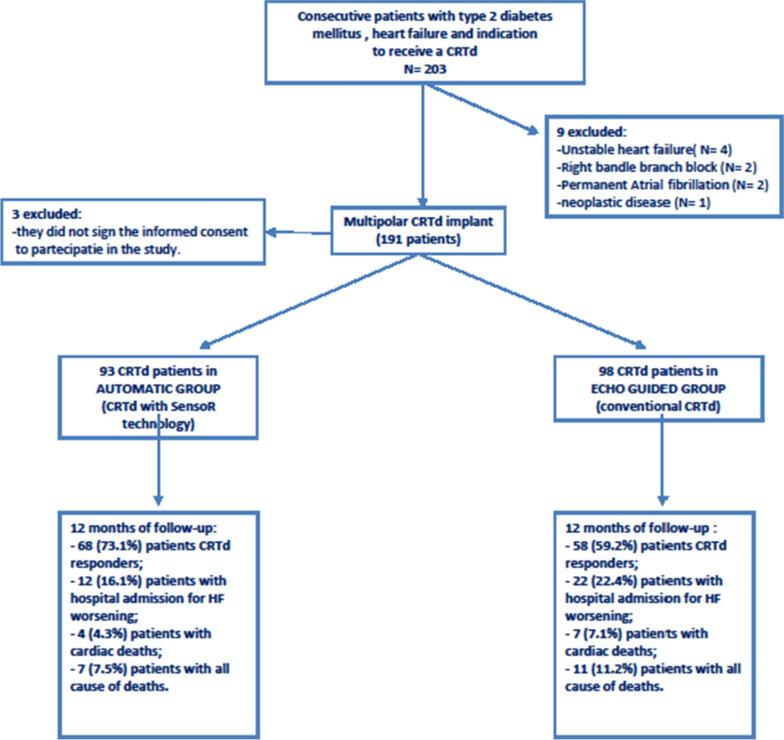
Methods: We designed a prospective, multicenter study to recruit, from October 2016 to June 2019, 191 consecutive failing heart patients with T2DM, and candidate to receive a CRTd. Study outcomes were CRTd responders rate, hospitalizations for heart failure (HF) worsening, cardiac deaths and all cause of deaths in T2DM patients treated with CRTd and randomly optimized via automatic (n 93) vs. echocardiography-guided (n 98) approach at 12 months of follow-up.
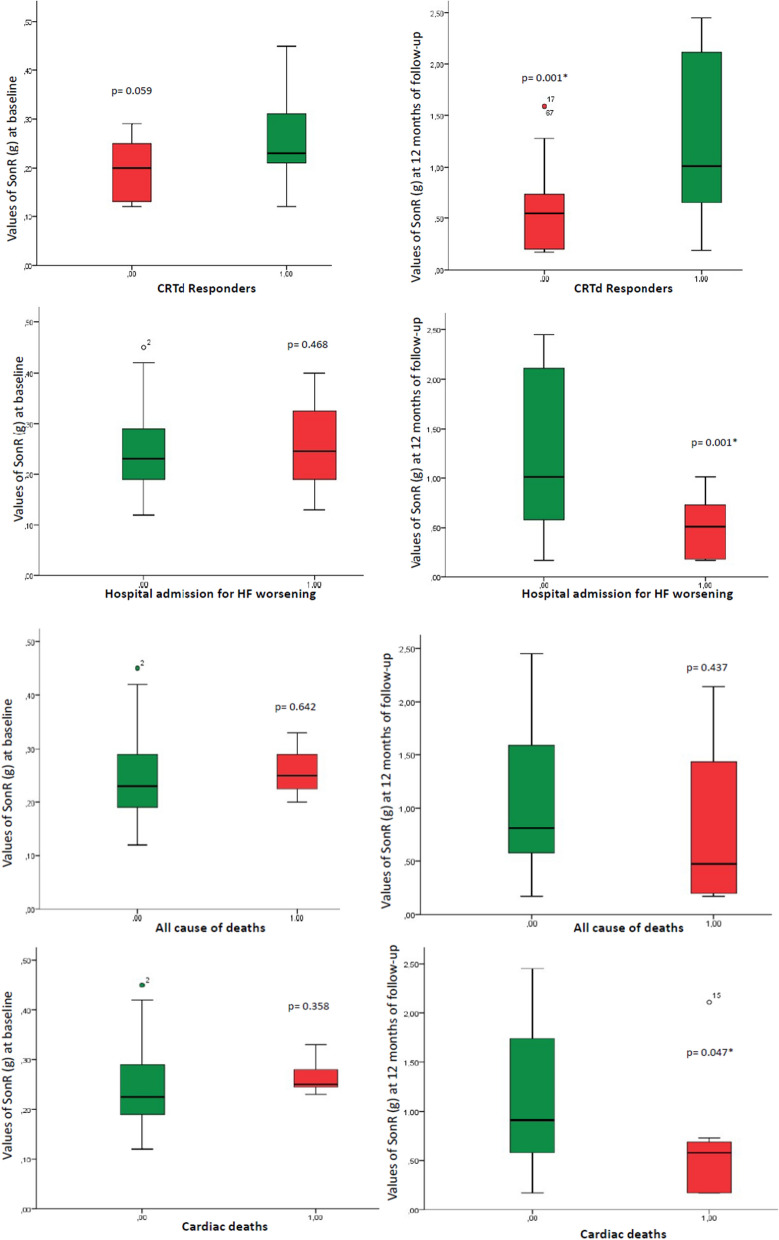
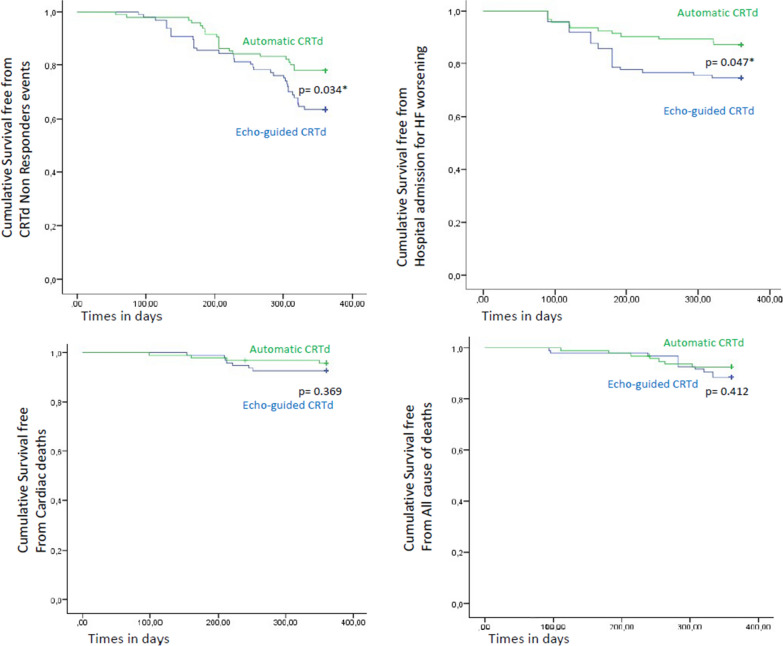
Results: We had a significant difference in the rate of CRTd responders (68 (73.1%) vs. 58 (59.2%), p 0.038), and hospitalizations for HF worsening (12 (16.1%) vs. 22 (22.4%), p 0.030) in automatic vs. echocardiography-guided group of patients. At multivariate Cox regression analysis, the automatic guided approach (3.636 [1.271-10.399], CI 95%, p 0.016) and baseline highest values of atrium pressure (automatic SonR values, 2.863 [1.537-6.231], CI 95%, p 0.006) predicted rate of CRTd responders. In automatic group, we had significant difference in SonR values comparing the rate of CRTd responders vs. non responders (1.24 ± 0.72 g vs. 0.58 ± 0.46 g (follow-up), p 0.001), the rate of hospitalizations for HF worsening events (0.48 ± 0.29 g vs. 1.18 ± 0.43 g, p 0.001), and the rate of cardiac deaths ( 1.13 ± 0.72 g vs. 0.65 ± 0.69 g, p 0.047).
Conclusions: Automatic optimization increased CRTd responders rate, and reduced hospitalizations for HF worsening. Intriguingly, automatic CRTd and highest baseline values of SonR could be predictive of CRTd responders. Notably, there was a significant difference in SonR values for CRTd responders vs. non responders, and about hospitalizations for HF worsening and cardiac deaths. Clinical trial ClinicalTrials.gov Identifier NCT04547244.
Keywords: Automatic CRTd optimization; Cardiac resynchronization therapy; Type 2 diabetes mellitus.
Conflict of interest statement
C.S edited and wrote the research project and the full manuscript.
Figures
References
-
- Sardu C, Barbieri M, Santamaria M, et al. Multipolar pacing by cardiac resynchronization therapy with a defibrillators treatment in type 2 diabetes mellitus failing heart patients: impact on responders rate, and clinical outcomes. Cardiovasc Diabetol. 2017;16(1):75. doi: 10.1186/s12933-017-0554-2. - DOI - PMC - PubMed
-
- Daubert C, Behar N, Raphael PM, Mabo P, Leclercq C. Avoiding non-responders to cardiac resynchronization therapy: a practical guide. Eur Heart J. 2017;38:1463–1472. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
