

Association Between Filgrastim Biosimilar Availability and Changes in Claim Payments and Patient Out-of-Pocket Costs for Biologic Filgrastim Products
- PMID: 33248515
- PMCID: PMC7748066
- DOI: 10.1016/j.jval.2020.06.014
Association Between Filgrastim Biosimilar Availability and Changes in Claim Payments and Patient Out-of-Pocket Costs for Biologic Filgrastim Products
Abstract
Objectives: To estimate the effect of filgrastim-sndz market entry on patient out-of-pocket costs and claim payments for filgrastim products.
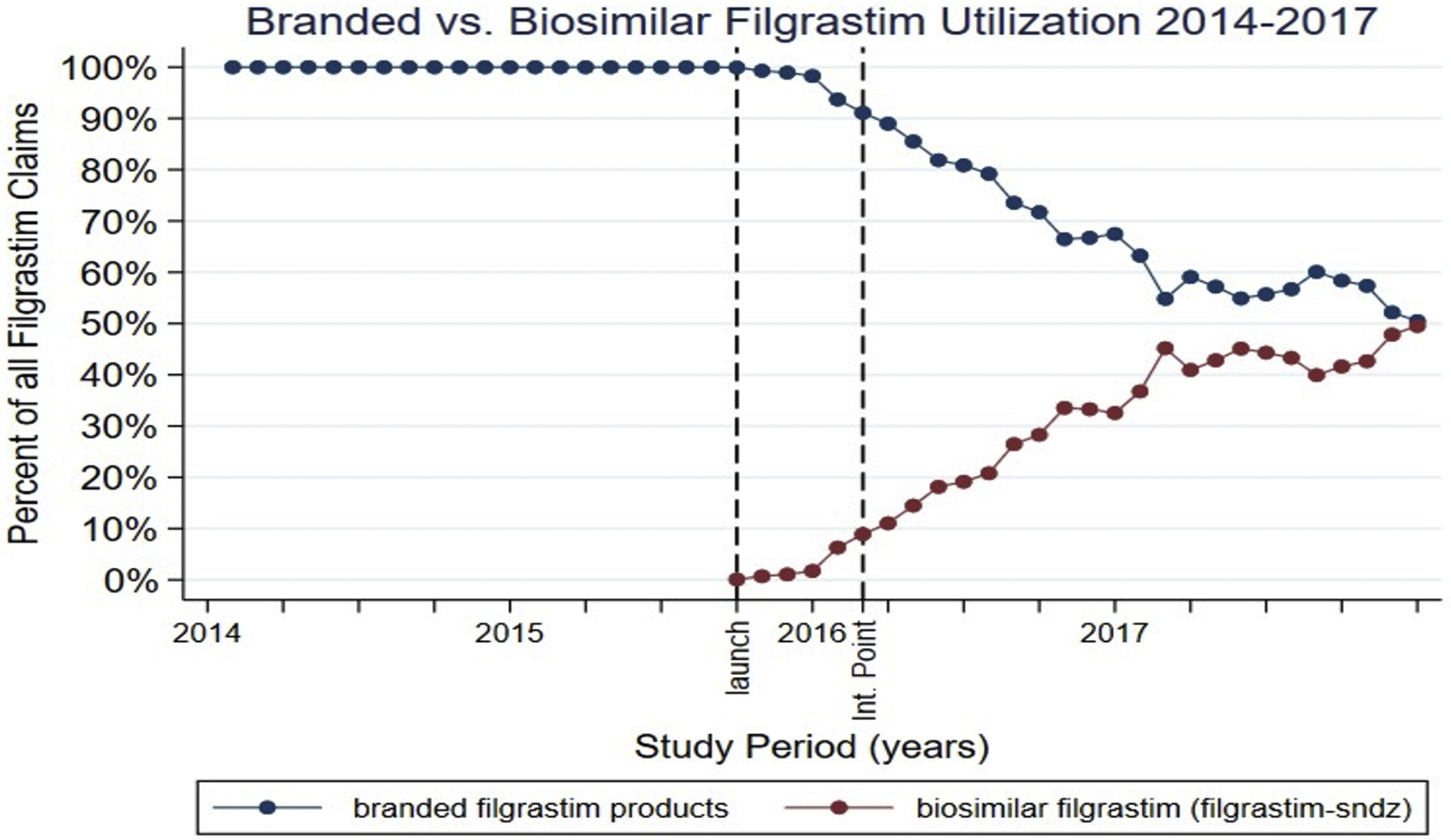
Methods: This study used a single interrupted time series design with longitudinal, nationally representative, individual-level claims data from IBM MarketScan. Analyses included all outpatient and prescription claims for branded filgrastim (filgrastim and tbo-filgrastim) and biosimilar filgrastim (filgrastim-sndz) from January 1, 2014, to December 31, 2017. Outcomes of interest included changes in monthly claim payments and monthly patient out-of-pocket costs for filgrastim products.
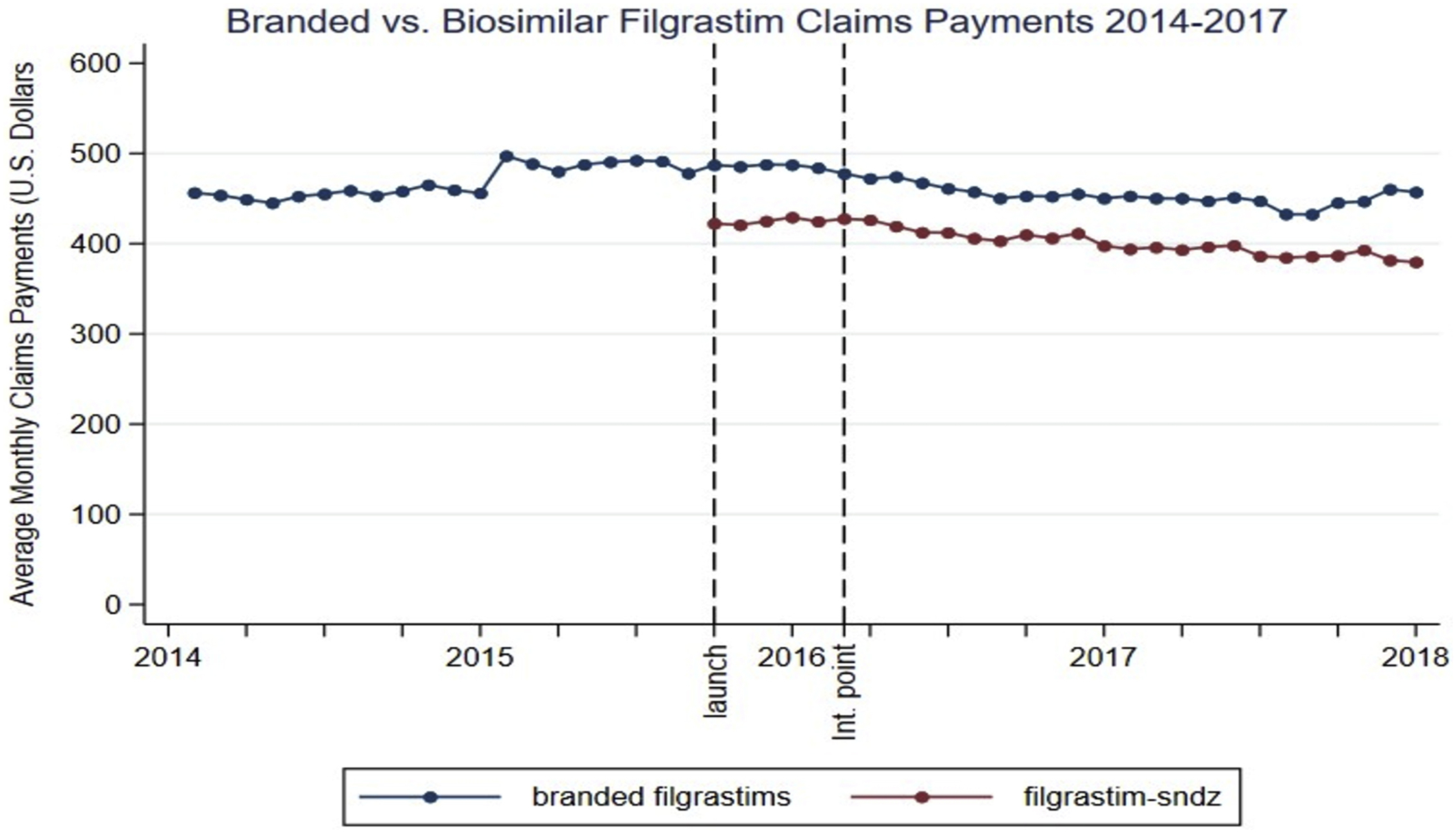
Results: In the baseline period (January 2014 to February 2016), insurers paid an average of $472.21 (95% confidence interval [CI]: 465.38-479.03) for 480 mcg of branded filgrastim, whereas patients paid an average of $49.26 (CI: 34.25-64.27). Filgrastim-sndz market entry was associated with a statistically significant and immediate 1-month decrease in insurer payment of $30.77 (95% CI: -40.59 to -20.94) and a significant decrease in monthly insurer payment trend of $3.10 per month (95% CI: -3.90 to -2.31) relative to baseline. Long-term changes in patient out-of-pocket costs were modest and restricted to beneficiaries enrolled in high cost sharing plans.
Conclusions: Biosimilar filgrastim availability led to significant immediate and long-term decreases in claims payments for filgrastim products, supporting efforts to facilitate biosimilar adoption in the United States. Nevertheless, there were only slight changes in patient out-of-pocket costs, restricted to beneficiaries enrolled in high cost sharing plans, suggesting the importance of further work assessing the relationship between biosimilar availability and patient out-of-pocket costs.
Keywords: biosimilars; commercial insurance; filgrastim; insurer payments; patient out-of-pocket costs.
Copyright © 2020 ISPOR–The Professional Society for Health Economics and Outcomes Research. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest Disclosures: Dr Alexander reported receiving personal fees from IQVIA Monument Analytics, and OptumRx outside the submitted work. Dr Alexander is the past Chair of FDA’s Peripheral and Central Nervous System Advisory Committee; has served as a paid advisor to IQVIA; is a co-founding Principal and equity holder in Monument Analytics, a healthcare consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation; and is a member of OptumRx’s National P&T Committee. This arrangement has been reviewed and approved by Johns Hopkins University in accordance with its conflict of interest policies.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
