

Use of cardiac CT amidst the COVID-19 pandemic and beyond: North American perspective
- PMID: 33248903
- PMCID: PMC7661966
- DOI: 10.1016/j.jcct.2020.11.004
Use of cardiac CT amidst the COVID-19 pandemic and beyond: North American perspective
Abstract
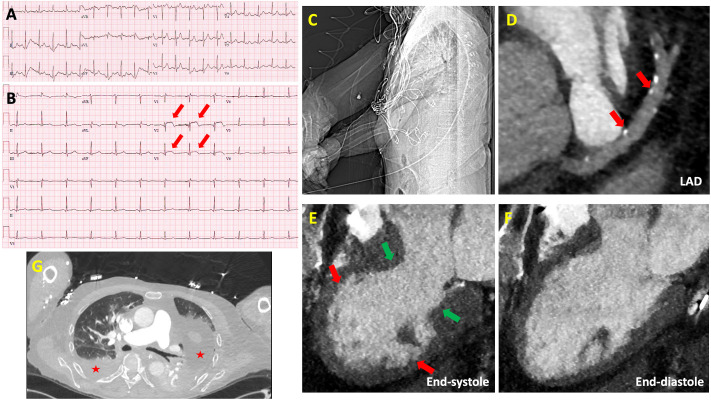
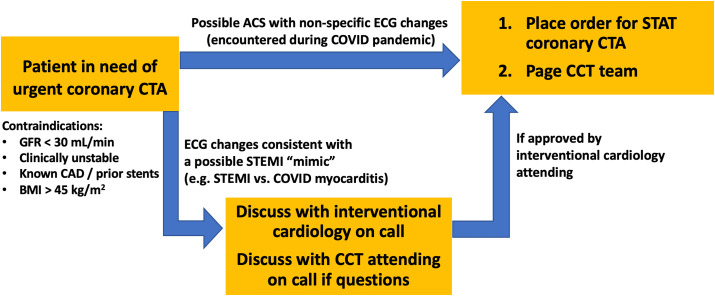
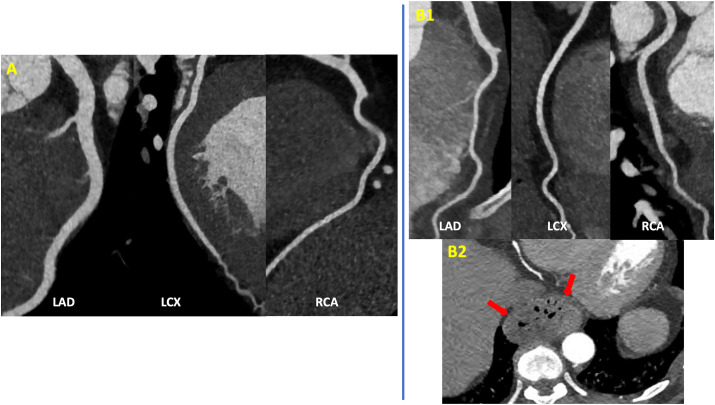
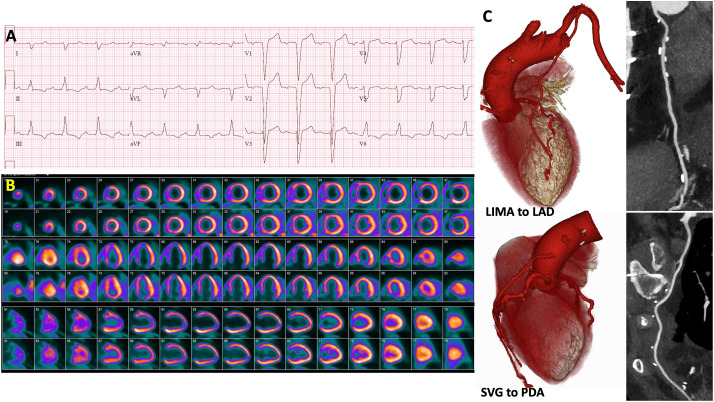
The COVID-19 pandemic has affected patient care deliver throughout the world, resulting in a greater emphasis on efficiently and safety. In this article, we discuss the experiences of several North American centers in utilizing cardiac CT during the pandemic. We also provide a case-based overview which highlights the advantages of cardiac CT in evaluating the following scenarios: (1) patients with possible myocardial injury versus myocardial infarction; (2) patients with acute chest pain; (3) patients with stable chest pain; (4) patients with possible intracardiac thrombus; (5) patients with valvular heart disease. For each scenario, we also provide an overview of various societies recommendations which have highlighted the use of cardiac CT during different phases of the COVID-19 pandemic. We hope that the advantages of cardiac CT that have been realized during the pandemic can help promote wider adoption of this technique and improved coverage and payment by payors.
Keywords: COVID-19; Cardiac CT; Coronary CTA.
Copyright © 2020 Society of Cardiovascular Computed Tomography. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest None of the authors of this manuscript have a conflict of interest relevant to this topic.
Figures


References
-
- Zoghbi William A., DiCarli Marcelo F., Blankstein Ron, Choi Andrew D., Flachskampf Frank A., Geske Jeffrey B., Grayburn Paul A., Jaffer Farouc A., Kwong Raymond Y., Jonathan A. 2020. Multimodality Cardiovascular Imaging in the Midst of the COVID-19 Pandemic: Ramping up Safely to a New Normal. JACC: Cardiovascular Imaging. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
