

Group-randomized trial of tailored brief shared decision-making to improve asthma control in urban black adults
- PMID: 33249632
- PMCID: PMC7902417
- DOI: 10.1111/jan.14646
Group-randomized trial of tailored brief shared decision-making to improve asthma control in urban black adults
Abstract
Aims: To assess the intervention effects of BREATHE (BRief intervention to Evaluate Asthma THErapy), a novel brief shared decision-making intervention and evaluate feasibility and acceptability of intervention procedures.
Design: Group-randomized longitudinal pilot study.
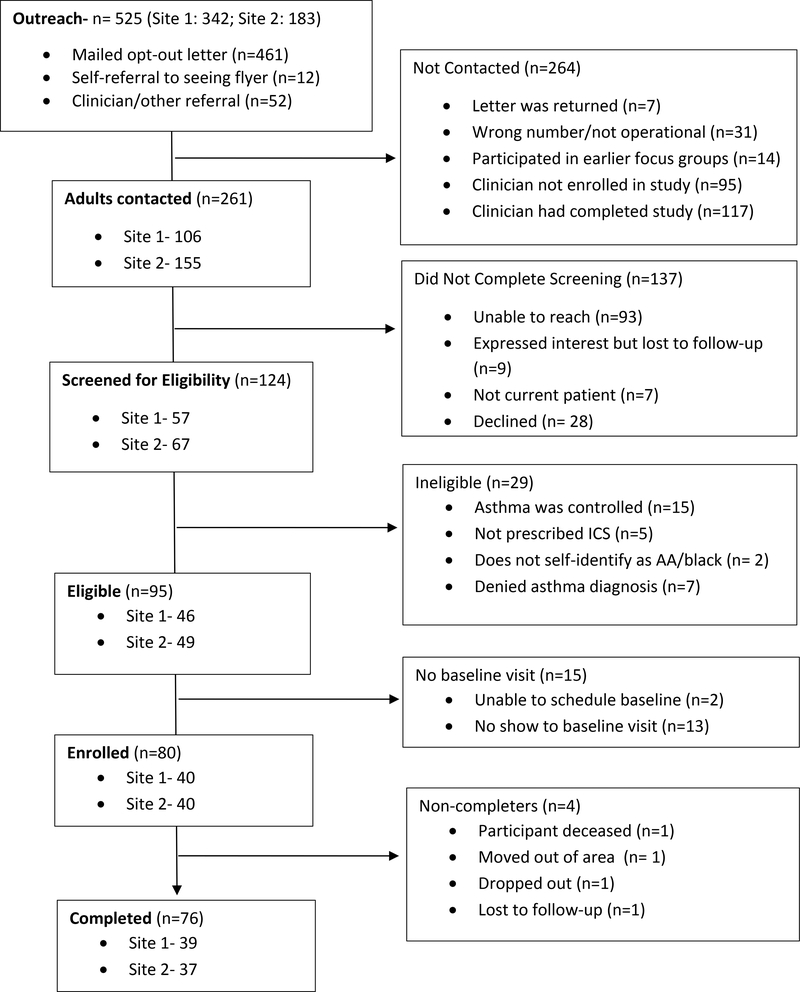
Methods: In total, 80 adults with uncontrolled persistent asthma participated in a trial comparing BREATHE (N = 40) to a dose-matched attention control intervention (N = 40). BREATHE is a one-time shared decision-making intervention delivered by clinicians during routine office visits. Ten clinicians were randomized and trained on BREATHE or the control condition. Participants were followed monthly for 3 months post-intervention. Data were collected from December 2017 - May 2019 and included surveys, lung function tests, and interviews.
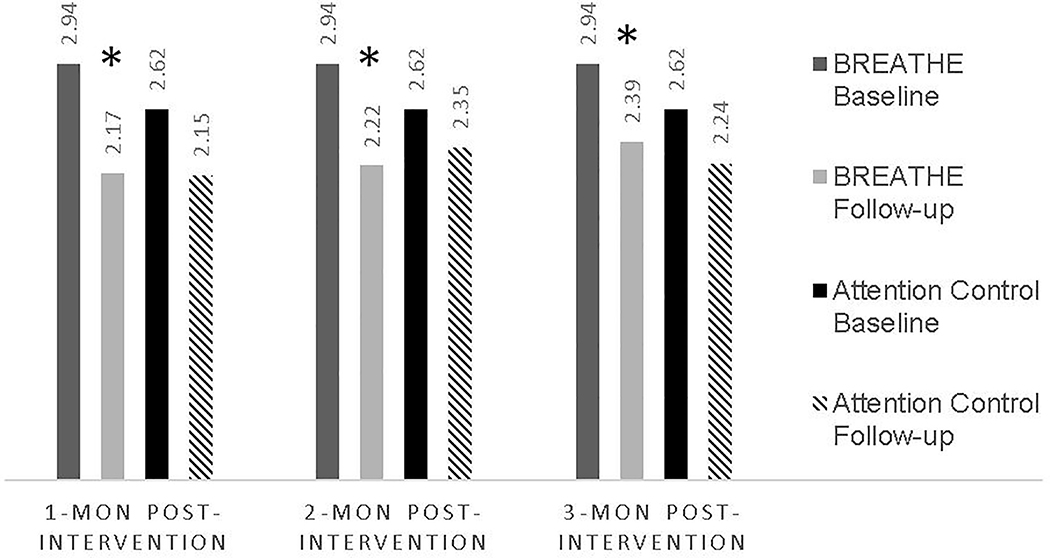
Results: Participants were Black/multiracial (100%) mostly female (83%) adults (mean age 45). BREATHE clinicians delivered BREATHE to all 40 participants with fidelity based on expert review of audiorecordings. While the control group reported improvements in asthma control at 1-month and 3-month follow-up, only BREATHE participants had better asthma control at each timepoint (β = 0.77; standard error (SE)[0.17]; p ≤ 0.0001; β = 0.71; SE[0.16]; p ≤ 0.0001; β = 0.54; SE[0.15]; p = .0004), exceeding the minimally important difference. BREATHE participants also perceived greater shared decision-making occurred during the intervention visit (β = 7.39; SE[3.51]; p = .03) and fewer symptoms at follow-up (e.g., fewer nights woken, less shortness of breath and less severity of symptoms) than the controls. Both groups reported improved adherence and fewer erroneous medication beliefs.
Conclusion: BREATHE is a promising brief tailored intervention that can be integrated into office visits using clinicians as interventionists. Thus, BREATHE offers a pragmatic approach to improving asthma outcomes and shared decision-making in a health disparity population.
Impact: The study addressed the important problem of uncontrolled asthma in a high-risk vulnerable population. Compared with the dose-matched attention control condition, participants receiving the novel brief tailored shared decision-making intervention had significant improvements in asthma outcomes and greater perceived engagement in shared decision-making. Brief interventions integrated into office visits and delivered by clinicians may offer a pragmatic approach to narrowing health disparity gaps. Future studies where other team members (e.g., office nurses, social workers) are trained in shared decision-making may address important implementation science challenges as it relates to adoption, maintenance, and dissemination. TRAIL REGISTRATION: clinicaltrials.gov # NCT03300752.
目的: 评估呼吸 (评估哮喘治疗的简短干预) 的干预效果, 一种新颖的简短共同决策干预, 并评估干预程序的可行性和可接受性。 设计: 分组随机纵向试点研究。 方法: 总共有80名患有不受控持续性哮喘的成人参与了一项对照呼吸 (N=40) 和剂量匹配的注意力控制干预 (N=40)试验。呼吸是临床医生在常规的门诊就诊中提供的一次性共同决策干预。10名临床医生被随机分配并接受呼吸或对照条件的培训。受试者在干预后的3个月内每月接受一次随访。数据收集于2017年12月至2019年5月, 其中包括调查、肺功能测试和访谈。 结果: 参与者为黑人/多种族 (100%) , 大部分为女性 (83%)成人 (平均年龄45岁) 。呼吸临床医生根据专家对录音的回顾, 准确地为所有40名参与者提供了呼吸服务。尽管对照组在1个月和3个月的随访中报告了哮喘控制的改善, 但只有呼吸参与者在每个时间点有更好的哮喘控制(β=0.77; 标准误差 (SE)【0.17】;p≤0.0001;β=0.71;SE【0.16】;p≤0.0001;β=0.54;SE【0.15】;p=.0004) , 超过了最小重要差异。与对照组相比, 呼吸参与者还认为在干预访视期间, 发生了更多的共同决策, (β=7.39;SE【3.51】;p=0.03) , 随访时症状出现地更少 (例如, 醒夜更少, 呼吸急促更少, 症状较轻) 。两组患者的依从性均有所改善, 错误的用药观念也有所减少。 结论: 呼吸是一种有效的短期定制干预, 可将临床医生作为干预与门诊就诊结合使用。因此, 呼吸提供了一个务实的方法来改善哮喘的结果和健康不平等人群的共同决策。 影响: 本项研究解决了高危易感人群中失控哮喘的重要问题。与剂量匹配的注意力控制条件相比, 接受新简短定制的共同决策干预的参与者在哮喘转归方面有显著改善, 且其在共同决策方面有更大的参与度。将简短的干预措施纳入到门诊就诊中, 并由临床医生提供, 可能提供缩小健康差距的务实方法。在未来的研究中, 其他团队成员 (如办公室护士、社会工作者) 将接受共同决策方面的培训, 这可能会解决实施科学在采用、维护和传播方面的重要挑战。 试验注册: clinicaltrials.gov # NCT03300752.
Keywords: adherence; community-engaged research; disease management; health beliefs; implementation science; minority; motivational interviewing; nursing; pragmatic.
© 2020 John Wiley & Sons Ltd.
Conflict of interest statement
No conflict of interest has been declared by the authors.
Figures
References
-
- Battersby M, Von Korff M, Schaefer J,. Davis C, Ludman E, Greene SM, Parkerton M, & Wagner E,H (2010). Twelve evidence-based principles for implementing self-management support in primary care. Joint Commission Journal of Quality and Patient Safety, 36(12), 561–570. 10.1016/S1553-7250(10)36084-3 - DOI - PubMed
-
- Bellg AJ, Borrelli B, Resnick B, Hecht J, Minicucci DS, Ory M, Ogedegbe G, Orwig D, Ernst D, Czajkowski S; Treatment Fidelity Workgroup of the NIH Behavior Change Consortium. (2004). Enhancing treatment fidelity in health behavior change studies: Best practices and recommendations from the NIH Behavior Change Consortium. Health Psychology, 23(5), 443–451. 10.1037/0278-6133.23.5.443 - DOI - PubMed
