

Progression of Beat-to-Beat Blood Pressure Variability Despite Best Medical Management
- PMID: 33249860
- PMCID: PMC7720874
- DOI: 10.1161/HYPERTENSIONAHA.120.16290
Progression of Beat-to-Beat Blood Pressure Variability Despite Best Medical Management
Abstract
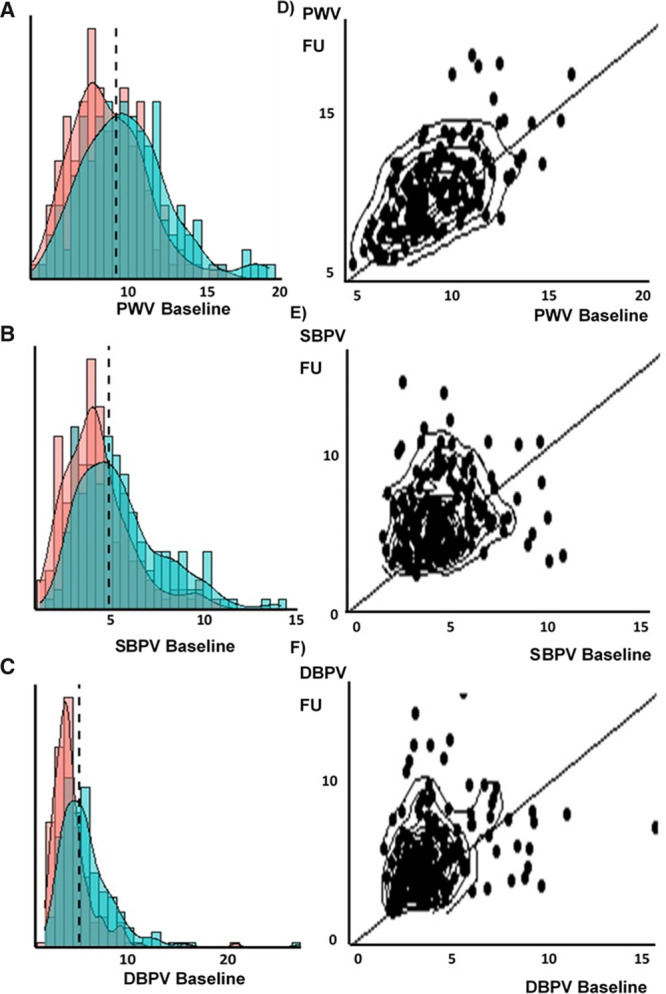
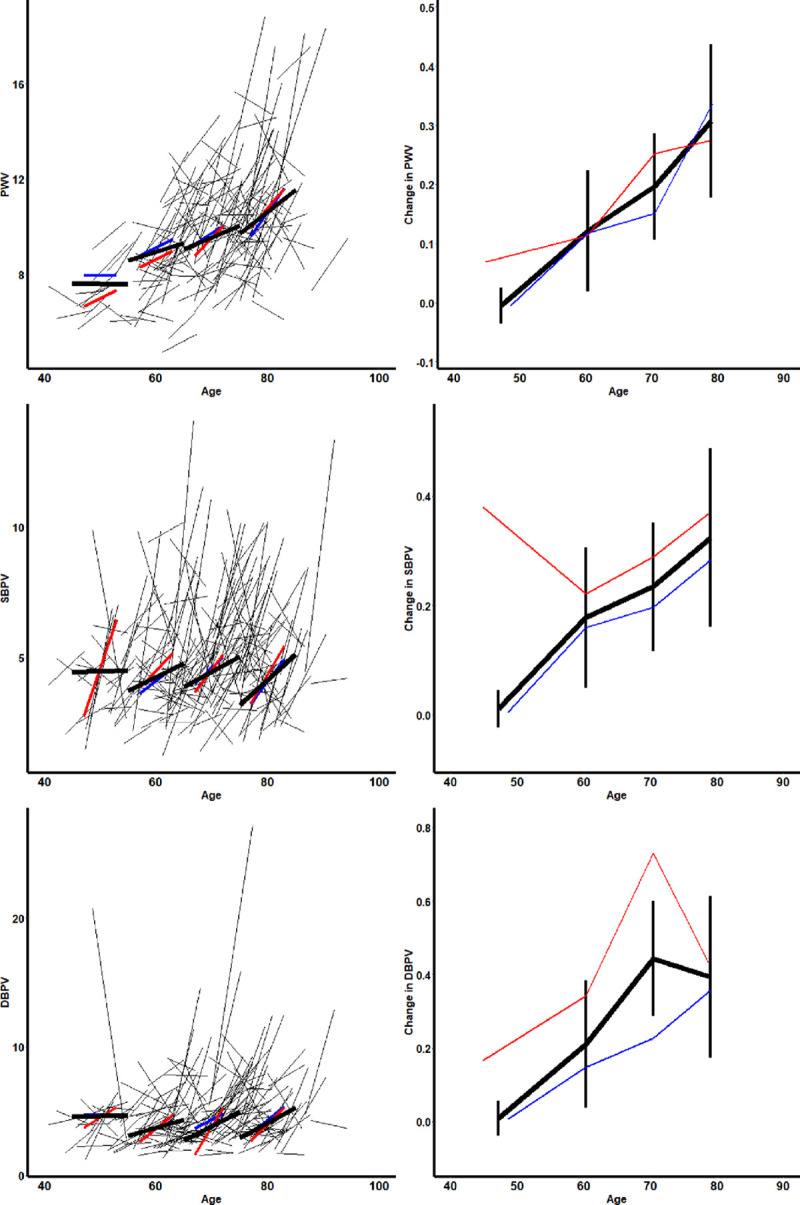
Beat-to-beat variability in blood pressure (BP) is associated with recurrent stroke despite good control of hypertension. However, no study has identified rates of progression of beat-to-beat BP variability (BPV), its determinants, or which patient groups are particularly affected, limiting understanding of its potential as a treatment target. In consecutive patients one month after a transient ischaemic attack or nondisabling stroke (Oxford Vascular Study), continuous noninvasive BP was measured beat-to-beat over 5 minutes (Finometer). Arterial stiffness was measured by carotid-femoral pulse wave velocity (Sphygmocor). Repeat assessments were performed at the 5-year follow-up visit and agreement determined by intraclass correlation coefficient. Rates of progression of systolic BPV (SBPV) and diastolic BPV (DBPV) and their determinants were estimated by mixed-effect linear models, adjusted for age, sex, and cardiovascular risk factors. One hundred eighty-eight of 310 surviving, eligible patients had repeat assessments after a median of 5.8 years. Pulse wave velocity was highly reproducible but SBPV and DBPV were not (intraclass correlation coefficient: 0.71, 0.10, and 0.16, respectively), however, all 3 progressed significantly (pulse wave velocity, 2.39%, P<0.0001; SBPV, 8.36%, P<0.0001; DBPV, 9.7, P<0.0001). Rate of progression of pulse wave velocity, SBPV, and DBPV all increased significantly with age (P<0.0001), with an increasingly positive skew and were particularly associated with female sex (pulse wave velocity P=0.00035; SBPV P<0.0001; DBPV P<0.0001) and aortic mean SBP (SBPV P=0.037, DBPV P<0.0001). Beat-to-beat BP variability progresses significantly in high-risk patients, particularly in older individuals with elevated aortic systolic pressure. Beat-to-beat BPV and its progression represent potential new therapeutic targets to reduce cardiovascular risk.
Keywords: blood pressure; hypertension; linear models; prognosis; risk factors.
Figures
References
-
- Rothwell PM, Howard SC, Dolan E, O’Brien E, Dobson JE, Dahlöf B, Poulter NR, Sever PS; ASCOT-BPLA and MRC Trial Investigators. Effects of beta blockers and calcium-channel blockers on within-individual variability in blood pressure and risk of stroke. Lancet Neurol. 2010;9:469–480. doi: 10.1016/S1474-4422(10)70066-1 - PubMed
-
- Rothwell PM. Limitations of the usual blood-pressure hypothesis and importance of variability, instability, and episodic hypertension. Lancet. 2010;375:938–948. doi: 10.1016/S0140-6736(10)60309-1 - PubMed
-
- Webb AJ, Fischer U, Mehta Z, Rothwell PM. Effects of antihypertensive-drug class on interindividual variation in blood pressure and risk of stroke: a systematic review and meta-analysis. Lancet. 2010;375:906–915. doi: 10.1016/S0140-6736(10)60235-8 - PubMed
-
- Muntner P, Whittle J, Lynch AI, Colantonio LD, Simpson LM, Einhorn PT, Levitan EB, Whelton PK, Cushman WC, Louis GT, et al. Visit-to-visit variability of blood pressure and coronary heart disease, stroke, heart failure, and mortality: a cohort study. Ann Intern Med. 2015;163:329–338. doi: 10.7326/M14-2803 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
