

Is a timely assessment of the hematocrit necessary for cardiovascular magnetic resonance-derived extracellular volume measurements?
- PMID: 33250055
- PMCID: PMC7702722
- DOI: 10.1186/s12968-020-00689-x
Is a timely assessment of the hematocrit necessary for cardiovascular magnetic resonance-derived extracellular volume measurements?
Abstract
Background: Cardiovascular magnetic resonance (CMR)-derived extracellular volume (ECV) requires a hematocrit (Hct) to correct contrast volume distributions in blood. However, the timely assessment of Hct can be challenging and has limited the routine clinical application of ECV. The goal of the present study was to evaluate whether ECV measurements lead to significant error if a venous Hct was unavailable on the day of CMR.
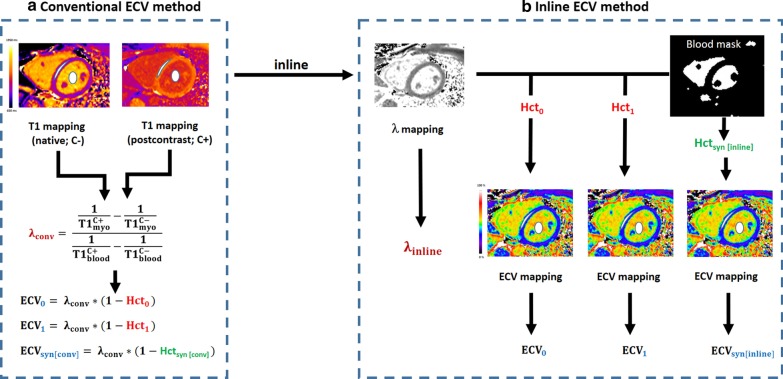
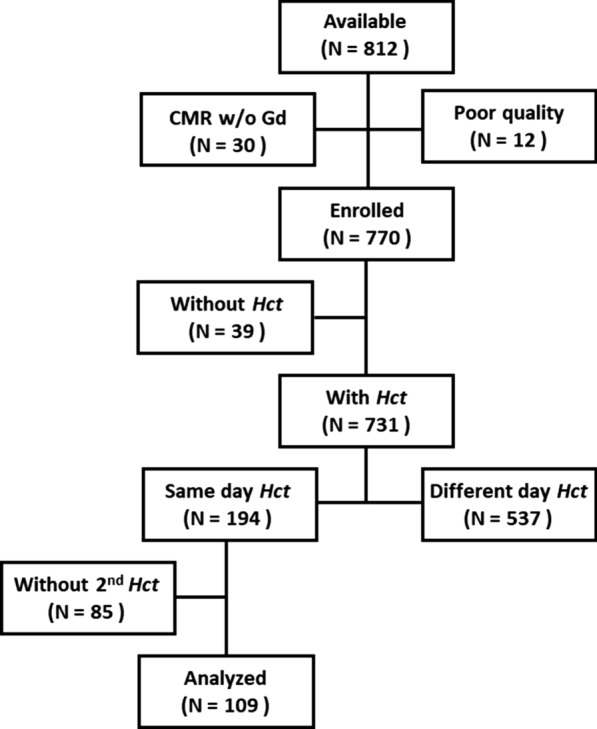
Methods: 109 patients with CMR T1 mapping and two venous Hcts (Hct0: a Hct from the day of CMR, and Hct1: a Hct from a different day) were retrospectively identified. A synthetic Hct (Hctsyn) derived from native blood T1 was also assessed. The study used two different ECV methods, (1) a conventional method in which ECV was estimated from native and postcontrast T1 maps using a region-based method, and (2) an inline method in which ECV was directly measured from inline ECV mapping. ECVs measured with Hct0, Hct1, and Hctsyn were compared for each method, and the reference ECV (ECV0) was defined using the Hct0. The error between synthetic (ECVsyn) and ECV0was analyzed for the two ECV methods.
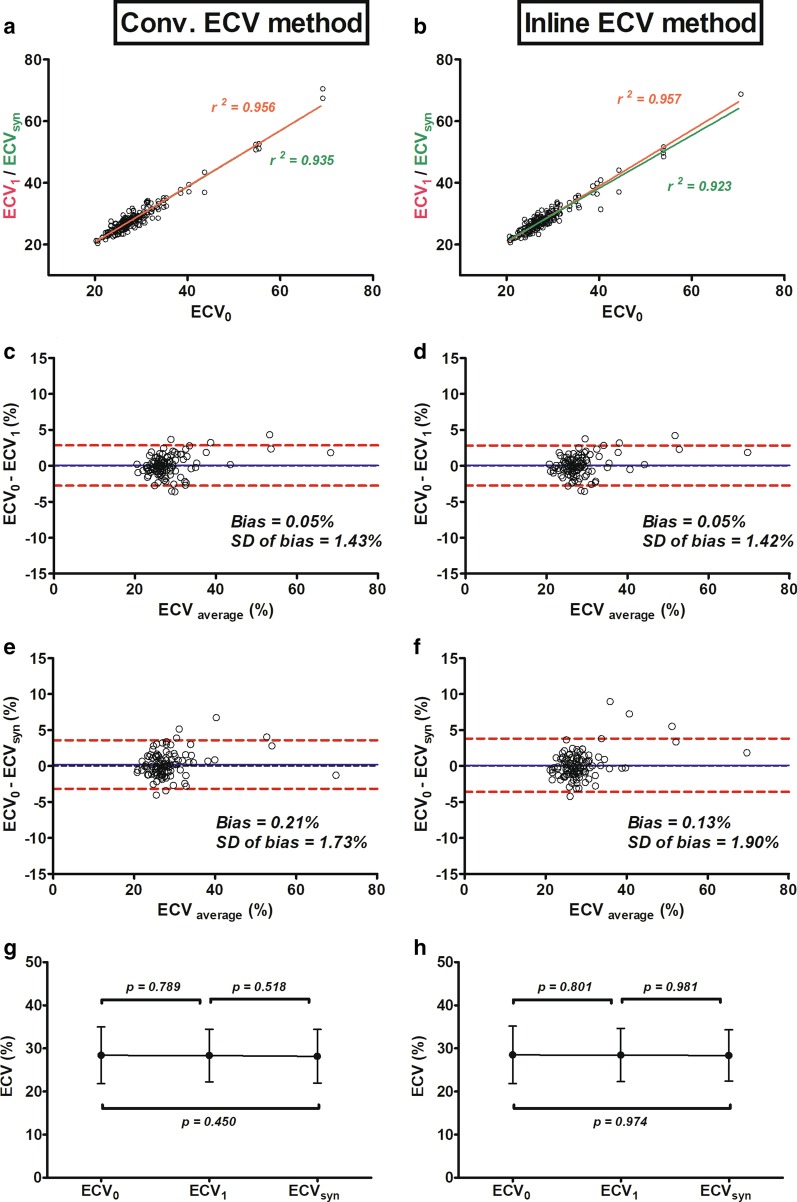
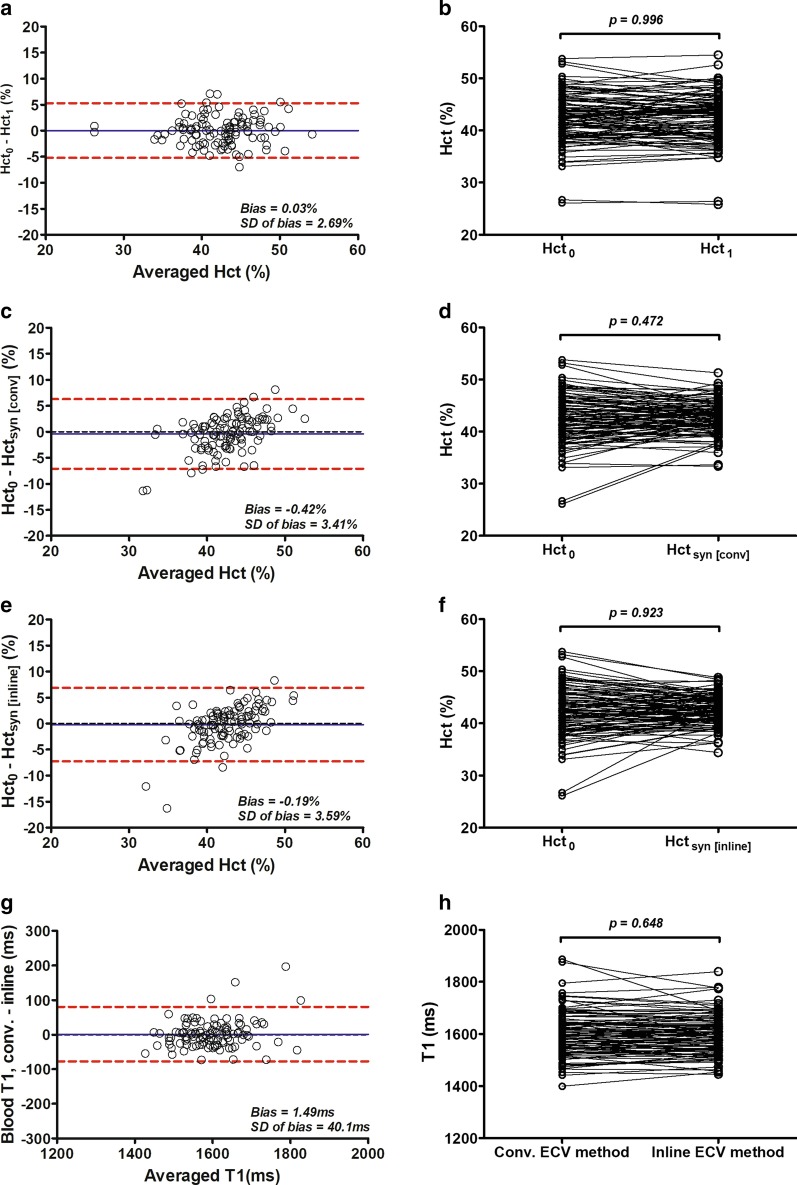
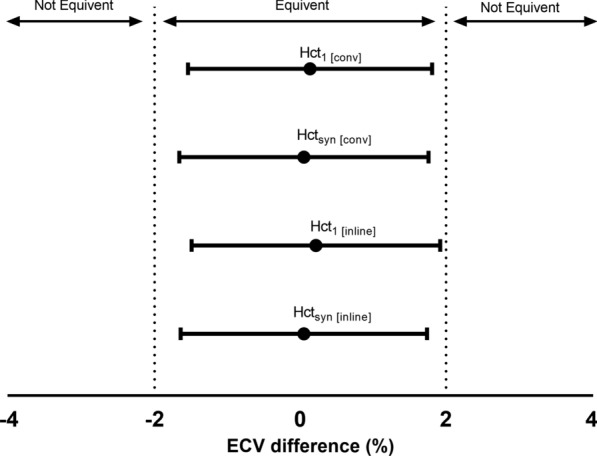
Results: ECV measured using Hct1 and Hctsyn were significantly correlated with ECV0 for each method. No significant differences were observed between ECV0 and ECV measured with Hct1 (ECV1; 28.4 ± 6.6% vs. 28.3 ± 6.1%, p = 0.789) and between ECV0 and ECV calculated with Hctsyn (ECVsyn; 28.4 ± 6.6% vs. 28.2 ± 6.2%, p = 0.45) using the conventional method. Similarly, ECV0 was not significantly different from ECV1 (28.5 ± 6.7% vs. 28.5 ± 6.2, p = 0.801) and ECVsyn (28.5 ± 6.7% vs. 28.4 ± 6.0, p = 0.974) using inline method. ECVsyn values revealed relatively large discrepancies in patients with lower Hcts compared with those with higher Hcts.
Conclusions: Venous Hcts measured on a different day from that of the CMR examination can still be used to measure ECV. ECVsyn can provide an alternative method to quantify ECV without needing a blood sample, but significant ECV errors occur in patients with severe anemia.
Keywords: Cardiovascular magnetic resonance; Extracellular volume fraction; Hematocrit; T1 mapping.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Messroghli DR, Moon JC, Ferreira VM, et al. Clinical recommendations for cardiovascular magnetic resonance mapping of T1, T2, T2* and extracellular volume: a consensus statement by the Society for Cardiovascular Magnetic Resonance (SCMR) endorsed by the European Association for Cardiovascular Imaging (EACVI) J Cardiovasc Magn Reson. 2017;19:75. doi: 10.1186/s12968-017-0389-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
