

Augmenting Anticancer Immunity Through Combined Targeting of Angiogenic and PD-1/PD-L1 Pathways: Challenges and Opportunities
- PMID: 33250900
- PMCID: PMC7674951
- DOI: 10.3389/fimmu.2020.598877
Augmenting Anticancer Immunity Through Combined Targeting of Angiogenic and PD-1/PD-L1 Pathways: Challenges and Opportunities
Abstract
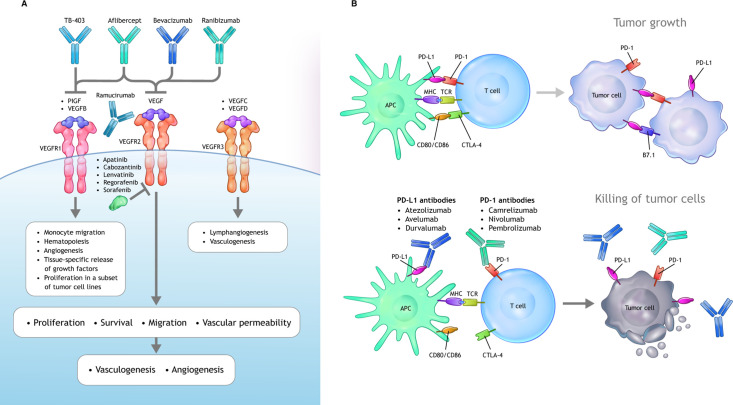
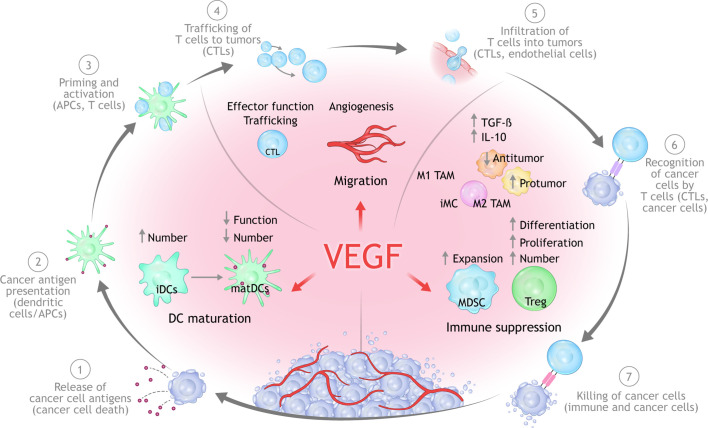
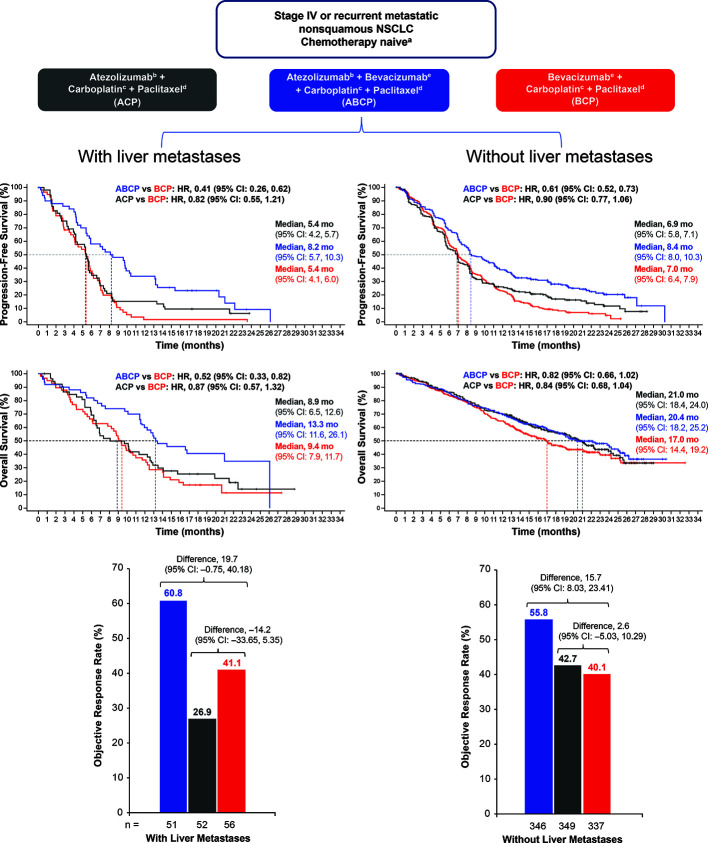
Cancer immunotherapy (CIT) with antibodies targeting the programmed cell death 1 protein (PD-1)/programmed cell death 1 ligand 1 (PD-L1) axis have changed the standard of care in multiple cancers. However, durable antitumor responses have been observed in only a minority of patients, indicating the presence of other inhibitory mechanisms that act to restrain anticancer immunity. Therefore, new therapeutic strategies targeted against other immune suppressive mechanisms are needed to enhance anticancer immunity and maximize the clinical benefit of CIT in patients who are resistant to immune checkpoint inhibition. Preclinical and clinical studies have identified abnormalities in the tumor microenvironment (TME) that can negatively impact the efficacy of PD-1/PD-L1 blockade. Angiogenic factors such as vascular endothelial growth factor (VEGF) drive immunosuppression in the TME by inducing vascular abnormalities, suppressing antigen presentation and immune effector cells, or augmenting the immune suppressive activity of regulatory T cells, myeloid-derived suppressor cells, and tumor-associated macrophages. In turn, immunosuppressive cells can drive angiogenesis, thereby creating a vicious cycle of suppressed antitumor immunity. VEGF-mediated immune suppression in the TME and its negative impact on the efficacy of CIT provide a therapeutic rationale to combine PD-1/PD-L1 antibodies with anti-VEGF drugs in order to normalize the TME. A multitude of clinical trials have been initiated to evaluate combinations of a PD-1/PD-L1 antibody with an anti-VEGF in a variety of cancers. Recently, the positive results from five Phase III studies in non-small cell lung cancer (adenocarcinoma), renal cell carcinoma, and hepatocellular carcinoma have shown that combinations of PD-1/PD-L1 antibodies and anti-VEGF agents significantly improved clinical outcomes compared with respective standards of care. Such combinations have been approved by health authorities and are now standard treatment options for renal cell carcinoma, non-small cell lung cancer, and hepatocellular carcinoma. A plethora of other randomized studies of similar combinations are currently ongoing. Here, we discuss the principle mechanisms of VEGF-mediated immunosuppression studied in preclinical models or as part of translational clinical studies. We also discuss data from recently reported randomized clinical trials. Finally, we discuss how these concepts and approaches can be further incorporated into clinical practice to improve immunotherapy outcomes for patients with cancer.
Keywords: angiogenesis; checkpoint inhibitor; programmed death ligand 1 (PD-L1); programmed death-1 (PD-1); tumor microenvironment; vascular endothelial growth factor (VEGF).
Copyright © 2020 Hack, Zhu and Wang.
Figures
Similar articles
-
Therapeutic Implications of Tumor Microenvironment in Lung Cancer: Focus on Immune Checkpoint Blockade.Front Immunol. 2022 Jan 7;12:799455. doi: 10.3389/fimmu.2021.799455. eCollection 2021. Front Immunol. 2022. PMID: 35069581 Free PMC article. Review.
-
Combination of anti-angiogenic therapy and immune checkpoint blockade normalizes vascular-immune crosstalk to potentiate cancer immunity.Exp Mol Med. 2020 Sep;52(9):1475-1485. doi: 10.1038/s12276-020-00500-y. Epub 2020 Sep 11. Exp Mol Med. 2020. PMID: 32913278 Free PMC article. Review.
-
Co-delivery of axitinib and PD-L1 siRNA for the synergism of vascular normalization and immune checkpoint inhibition to boost anticancer immunity.J Nanobiotechnology. 2025 Mar 10;23(1):194. doi: 10.1186/s12951-025-03170-y. J Nanobiotechnology. 2025. PMID: 40059141 Free PMC article.
-
The integration of immune checkpoint inhibitors with VEGF targeted agents in advanced gastric and gastroesophageal adenocarcinoma: a review on the rationale and results of early phase trials.J Hematol Oncol. 2021 Jan 12;14(1):13. doi: 10.1186/s13045-021-01034-0. J Hematol Oncol. 2021. PMID: 33436042 Free PMC article.
-
LKB1 dictates sensitivity to immunotherapy through Skp2-mediated ubiquitination of PD-L1 protein in non-small cell lung cancer.J Immunother Cancer. 2024 Dec 18;12(12):e009444. doi: 10.1136/jitc-2024-009444. J Immunother Cancer. 2024. PMID: 39694700 Free PMC article.
Cited by
-
Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma.Nat Med. 2022 Aug;28(8):1599-1611. doi: 10.1038/s41591-022-01868-2. Epub 2022 Jun 23. Nat Med. 2022. PMID: 35739268
-
The expanding role for small molecules in immuno-oncology.Nat Rev Drug Discov. 2022 Nov;21(11):821-840. doi: 10.1038/s41573-022-00538-9. Epub 2022 Aug 18. Nat Rev Drug Discov. 2022. PMID: 35982333 Review.
-
Research advances in mechanism of antiangiogenic therapy combined with immune checkpoint inhibitors for treatment of non-small cell lung cancer.Front Immunol. 2023 Oct 16;14:1265865. doi: 10.3389/fimmu.2023.1265865. eCollection 2023. Front Immunol. 2023. PMID: 37915579 Free PMC article. Review.
-
The role of angiogenic growth factors in the immune microenvironment of glioma.Front Oncol. 2023 Sep 13;13:1254694. doi: 10.3389/fonc.2023.1254694. eCollection 2023. Front Oncol. 2023. PMID: 37790751 Free PMC article. Review.
-
Resistance to Immunotherapy: Mechanisms and Means for Overcoming.Adv Exp Med Biol. 2021;1342:45-80. doi: 10.1007/978-3-030-79308-1_2. Adv Exp Med Biol. 2021. PMID: 34972962
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials