

Malignancy in giant cell tumor of bone in the extremities
- PMID: 33251099
- PMCID: PMC7680773
- DOI: 10.1016/j.jbo.2020.100334
Malignancy in giant cell tumor of bone in the extremities
Abstract
Background: Malignancy in giant cell tumor of bone (GCTB) is a rare tumor with relevant literature being sparse. In primary malignant GCTB, distinct areas of benign GCTB are juxtaposed with high-grade sarcoma, while in secondary malignant GCTB sarcoma occurs at the site of previously managed GCTB. This study assesses the distinguishing characteristics of patients with this condition, the time interval for development of secondary malignant GCTB, the outcome of treatment, and explores factors associated with oncologic outcomes.
Methods: This is a retrospective case series of patients from a prospectively collected institutional musculoskeletal oncology database. From January 1998 to December 2016, 1365 patients were managed for extremity GCTBs. 32 (2.3%) patients had malignant GCTB, including 12 with primary malignant GCTB and 20 with secondary malignant GCTB. The study population comprised 18 males and 14 females presenting at a mean age of 33.7 years (±13.0) and followed for a mean of 9.5 years (±7.4). Data were collected on patient and treatment-related factors, and the occurrence of local recurrence, metastasis, and death. The time from the diagnosis of GCTB to the secondary malignant GCTB was defined as the latent period.
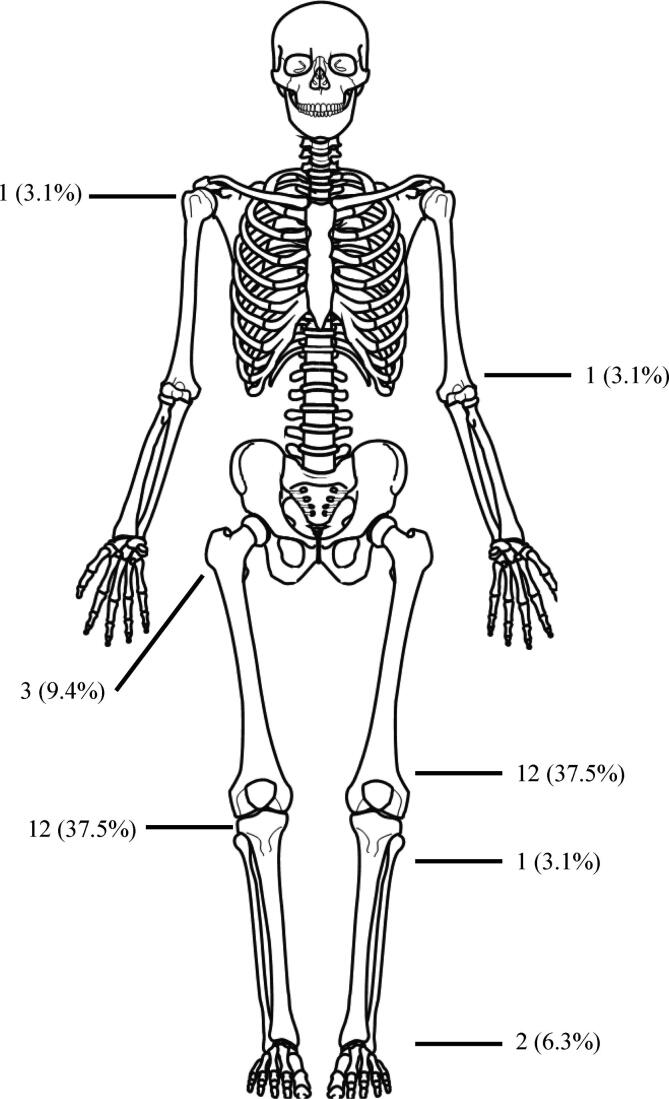
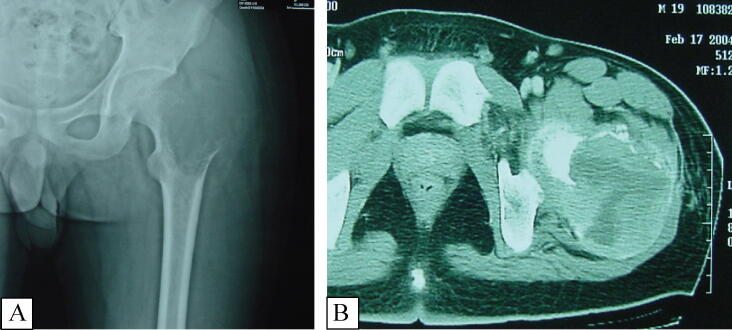
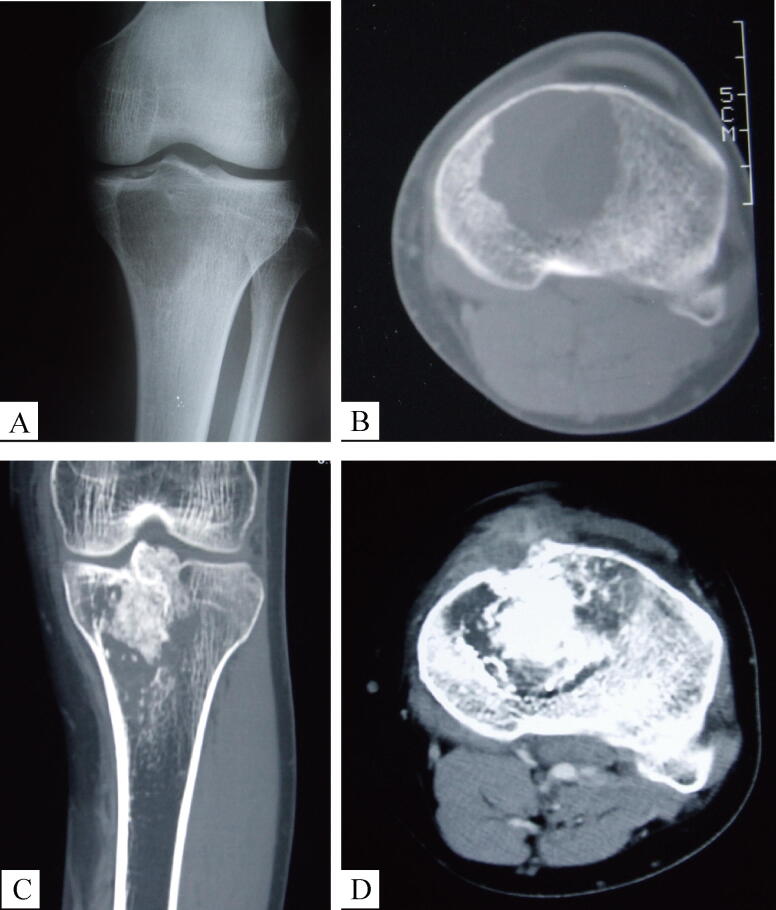
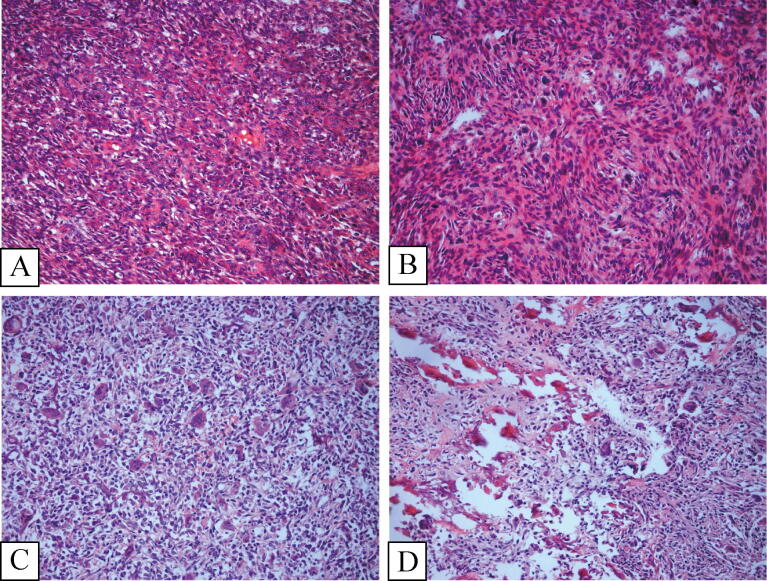
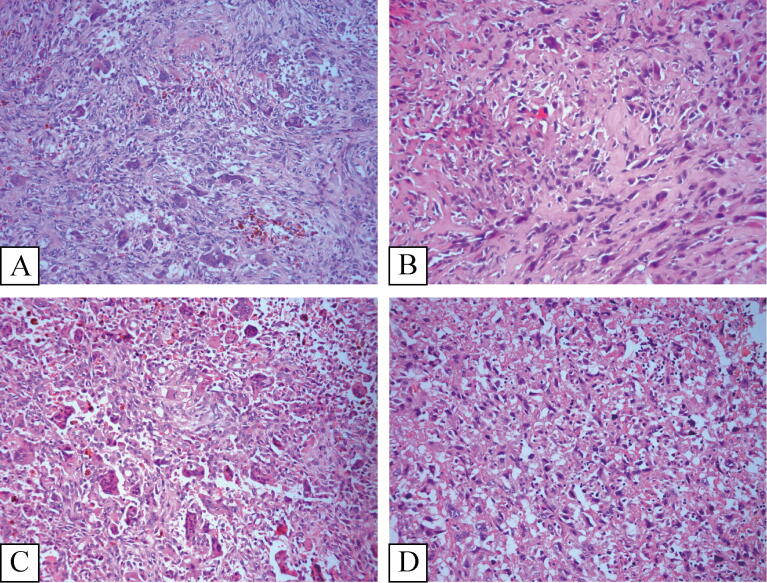
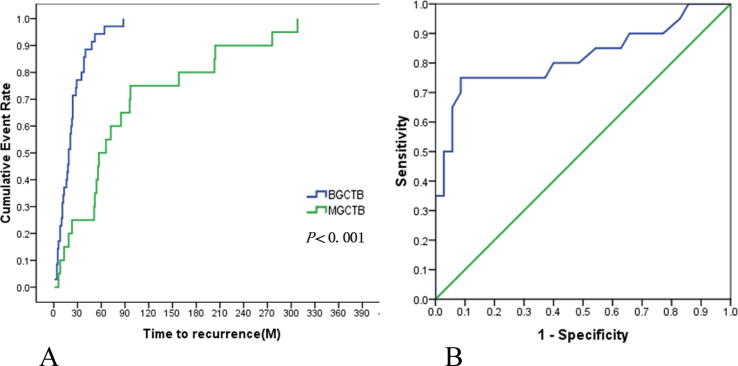
Results: Malignant GCTB most commonly presents in the distal femur and proximal tibia with pain and swelling. Radiologically, they are aggressive Campanacci Grade III tumors with prominent bony destruction and soft tissue extension. In the 20 patients with secondary malignant GCTB, the tumors were osteosarcoma in 15, undifferentiated pleomorphic sarcoma in 4 patients and fibrosarcoma in one patient. The mean latent period in patients with secondary malignant GCTB was 7.9 year (±7.3). The median recurrence-free survival (RFS) of secondary malignant GCTB (latent period) and benign GCTB were 61.5 and 19 months respectively (p < 0.001), receiver operating curve analysis found 49.5 months to be the critical threshold, with a longer interval to recurrence being seen in malignant recurrence. The 5 and 10-year overall survival rate of malignant GCTB were 45.8% and 36.1% respectively. The 5-year survival rates of primary malignant GCTB and secondary malignant GCTB were 56.2% and 40.0% respectively (p = 0.188). Adequate surgical margins decreased the local recurrence (LR) rate (P = 0.006). Pulmonary metastasis developed in 69% of patients. The median distant metastasis-free survival between malignant GCTB and benign GCTB were 9 and 21 months (p = 0.002). Chemotherapy was associated with a longer pulmonary metastasis free survival (13 months Vs 6 months, P = 0.002), but not with increased overall survival (57.0% Vs 33.3%, P = 0.167).
Conclusions: Malignant GCTB carries a poor prognosis. Accurate diagnosis is critical to avoid inadequate surgical margins when treating primary malignant GCTB. Aggressive tumors and pulmonary metastasis should raise suspicion for malignant GCTB. Secondary malignant transformation should be suspected in patients presenting with recurrence especially after 4 years. Adjuvant chemotherapy use did not benefit survival, but was associated with increased pulmonary progression-free survival.
Keywords: Bone; Chemotherapy; Giant cell tumor; Malignant; Recurrence; Survival.
© 2020 The Authors.
Figures
References
-
- Rock M.G., Sim F.H., Unni K.K., Witrak G.A., Frassica F.J., Schray M.F., Beabout J.W., Dahlin D.C. Secondary malignant giant-cell tumor of bone. Clinicopathological assessment of nineteen patients. J. Bone Joint Surg. Am. 1986;68:1073–1079. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
