

Classification of Progression Patterns in Glioblastoma: Analysis of Predictive Factors and Clinical Implications
- PMID: 33251147
- PMCID: PMC7673412
- DOI: 10.3389/fonc.2020.590648
Classification of Progression Patterns in Glioblastoma: Analysis of Predictive Factors and Clinical Implications
Abstract
Background: This study was designed to explore the progression patterns of IDH-wildtype glioblastoma (GBM) at first recurrence after chemoradiotherapy.
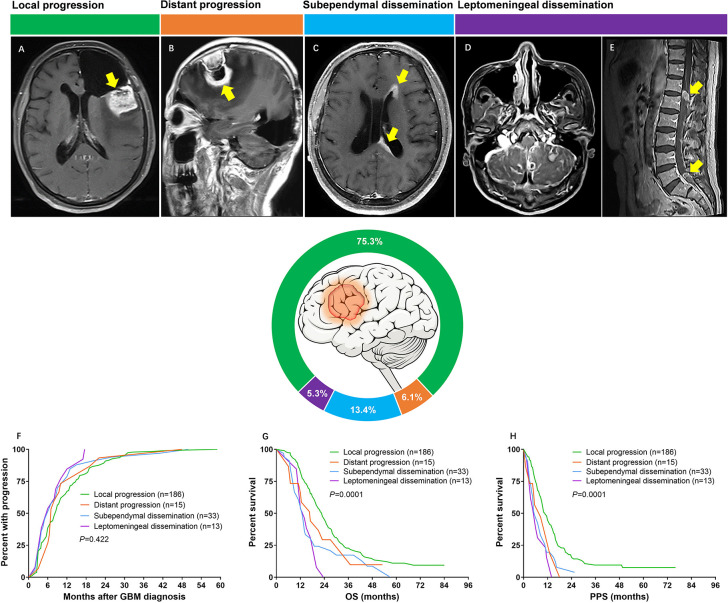
Methods: Records from 247 patients who underwent progression after diagnosis of IDH-wildtype GBM was retrospectively reviewed. Progression patterns were classified as either local, distant, subependymal or leptomeningeal dissemination based on the preoperative and serial postoperative radiographic images. The clinical and molecular characteristics of different progression patterns were analyzed.
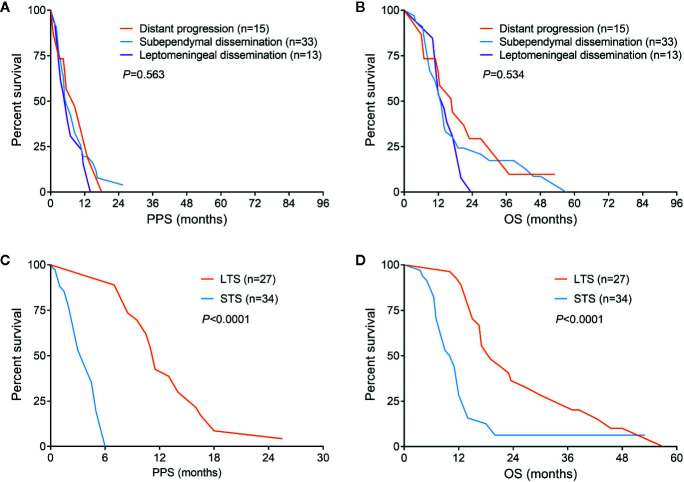
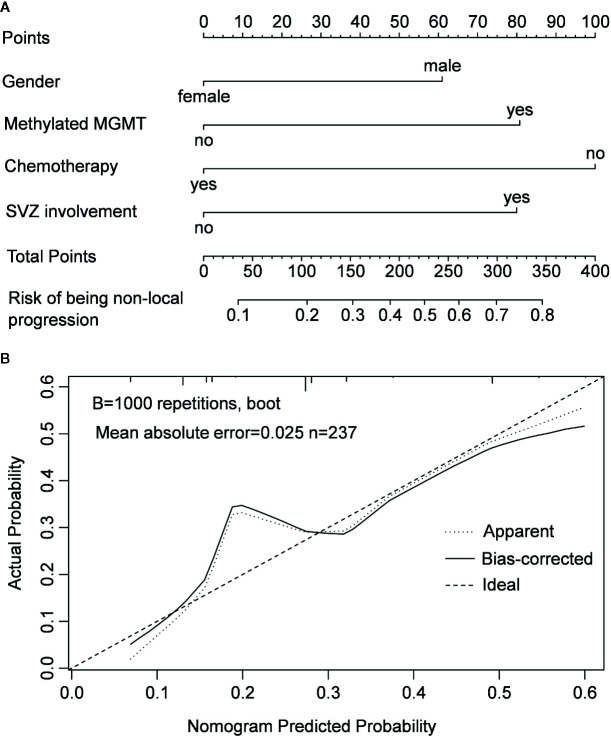
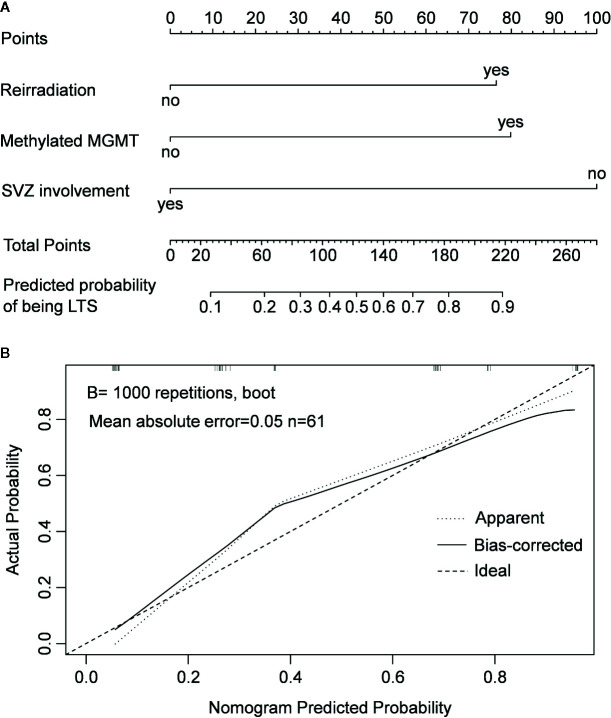
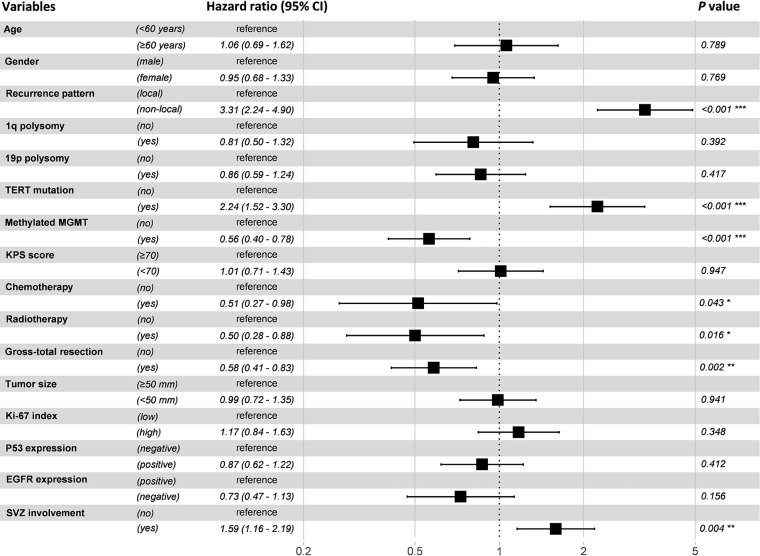
Results: A total of 186 (75.3%) patients had local progression, 15 (6.1%) patients had distant progression, 33 (13.3%) patients had subependymal dissemination, and 13 (5.3%) patients had leptomeningeal dissemination. The most favorable survival occurred in patients with local progression, while no significant difference of survival was found among patients with distant progression, subependymal or leptomeningeal dissemination who were thereby reclassified into non-local group. Multivariable analysis showed that chemotherapy was a protective factor for non-local progression, while gender of male, subventricular zone (SVZ) involvement and O6-methylguanine-DNA-methyltransferase (MGMT) promoter methylation were confirmed as risk factors for non-local progression (P < 0.05). Based on the factors screened by multivariable analysis, a nomogram was constructed which conferred high accuracy in predicting non-local progression. Patients in non-local group could be divided into long- and short-term survivors who differed in the rates of SVZ involvement, MGMT promoter methylation and reirradiation (P < 0.05), and a nomogram integrating these factors showed high accuracy in predicting long-term survivors.
Conclusion: Patients harboring different progression patterns conferred distinct clinical and molecular characteristics. Our nomograms could provide theoretical references for physicians to make more personalized and precise treatment decisions.
Keywords: glioblastoma; nomogram; prognosis; progression; subventricular zone.
Copyright © 2020 Jiang, Yu, Li, Cui, Ren, Yang, Zhao and Lin.
Figures
Similar articles
-
Differential Predictors and Clinical Implications Associated With Long-Term Survivors in IDH Wildtype and Mutant Glioblastoma.Front Oncol. 2021 May 13;11:632663. doi: 10.3389/fonc.2021.632663. eCollection 2021. Front Oncol. 2021. PMID: 34055603 Free PMC article.
-
Risk Factors of Distant Recurrence and Dissemination of IDH Wild-Type Glioblastoma: A Single-Center Study and Meta-Analysis.Cancers (Basel). 2024 Aug 18;16(16):2873. doi: 10.3390/cancers16162873. Cancers (Basel). 2024. PMID: 39199644 Free PMC article. Review.
-
Comparative Analysis of Subventricular Zone Glioblastoma Contact and Ventricular Entry During Resection in Predicting Dissemination, Hydrocephalus, and Survival.Neurosurgery. 2019 Nov 1;85(5):E924-E932. doi: 10.1093/neuros/nyz144. Neurosurgery. 2019. PMID: 31058968 Free PMC article.
-
Long-term outcomes of concomitant chemoradiotherapy with temozolomide for newly diagnosed glioblastoma patients: A single-center analysis.Medicine (Baltimore). 2017 Jul;96(27):e7422. doi: 10.1097/MD.0000000000007422. Medicine (Baltimore). 2017. PMID: 28682902 Free PMC article.
-
Relationships between recurrence patterns and subventricular zone involvement or CD133 expression in glioblastoma.J Neurooncol. 2020 Feb;146(3):489-499. doi: 10.1007/s11060-019-03381-y. Epub 2020 Feb 4. J Neurooncol. 2020. PMID: 32020479
Cited by
-
Comparing tumor microRNA profiles of patients with long‑ and short‑term‑surviving glioblastoma.Mol Med Rep. 2023 Jan;27(1):8. doi: 10.3892/mmr.2022.12895. Epub 2022 Nov 11. Mol Med Rep. 2023. PMID: 36367159 Free PMC article.
-
Targeting the neural stem cells in subventricular zone for the treatment of glioblastoma: an update from preclinical evidence to clinical interventions.Stem Cell Res Ther. 2023 May 11;14(1):125. doi: 10.1186/s13287-023-03325-4. Stem Cell Res Ther. 2023. PMID: 37170286 Free PMC article. Review.
-
Differential Predictors and Clinical Implications Associated With Long-Term Survivors in IDH Wildtype and Mutant Glioblastoma.Front Oncol. 2021 May 13;11:632663. doi: 10.3389/fonc.2021.632663. eCollection 2021. Front Oncol. 2021. PMID: 34055603 Free PMC article.
-
Concurrent chemoradiation and Tumor Treating Fields (TTFields, 200 kHz) for patients with newly diagnosed glioblastoma: patterns of progression in a single institution pilot study.J Neurooncol. 2022 Nov;160(2):345-350. doi: 10.1007/s11060-022-04146-w. Epub 2022 Nov 10. J Neurooncol. 2022. PMID: 36355259 Clinical Trial.
-
Location of Recurrences after Trimodality Treatment for Glioblastoma with Respect to the Delivered Radiation Dose Distribution and Its Influence on Prognosis.Cancers (Basel). 2023 May 30;15(11):2982. doi: 10.3390/cancers15112982. Cancers (Basel). 2023. PMID: 37296942 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Research Materials