

New-Onset Atrial Fibrillation After Coronary Artery Bypass Grafting and Long-Term Outcome: A Population-Based Nationwide Study From the SWEDEHEART Registry
- PMID: 33251914
- PMCID: PMC7955471
- DOI: 10.1161/JAHA.120.017966
New-Onset Atrial Fibrillation After Coronary Artery Bypass Grafting and Long-Term Outcome: A Population-Based Nationwide Study From the SWEDEHEART Registry
Abstract
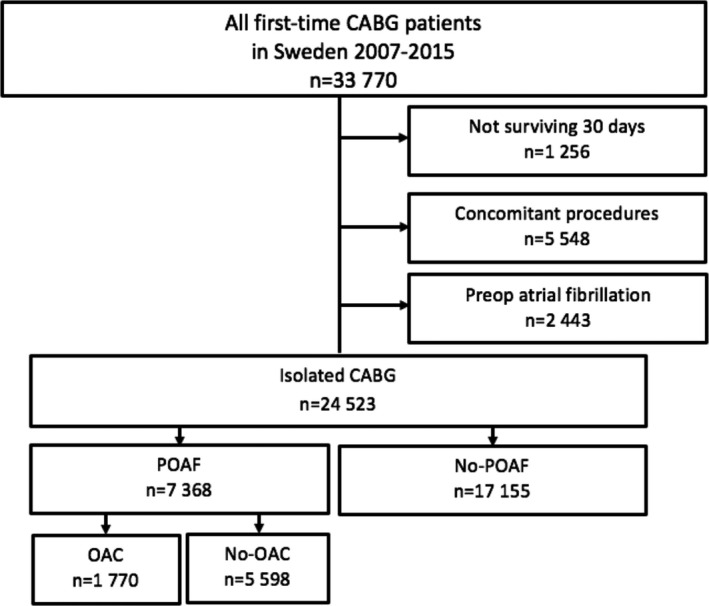
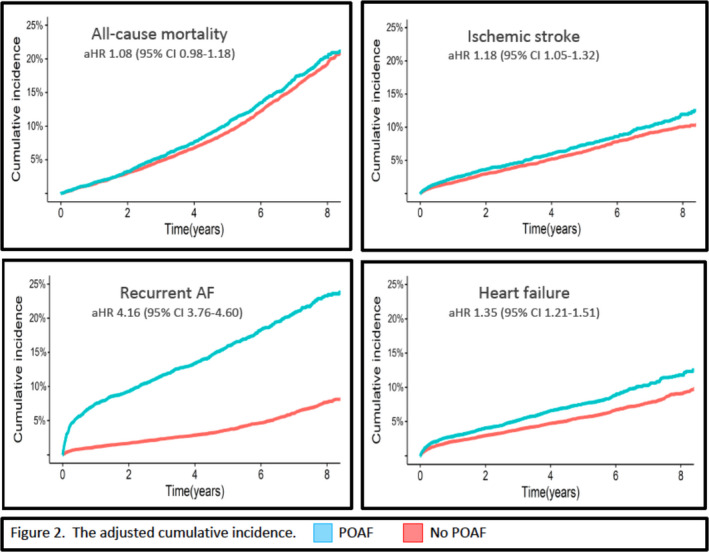
Background The long-term impact of new-onset postoperative atrial fibrillation (POAF) after coronary artery bypass grafting and the benefit of early-initiated oral anticoagulation (OAC) in patients with POAF are uncertain. Methods and Results All patients who underwent coronary artery bypass grafting without preoperative atrial fibrillation in Sweden from 2007 to 2015 were included in a population-based study using data from 4 national registries: SWEDEHEART (Swedish Web System for Enhancement and Development of Evidence-based Care in Heart Disease Evaluated According to Recommended Therapies), National Patient Registry, Dispensed Drug Registry, and Cause of Death Registry. POAF was defined as any new-onset atrial fibrillation during the first 30 postoperative days. Cox regression models (adjusted for age, sex, comorbidity, and medication) were used to assess long-term outcome in patients with and without POAF, and potential associations between early-initiated OAC and outcome. In a cohort of 24 523 patients with coronary artery bypass grafting, POAF occurred in 7368 patients (30.0%), and 1770 (24.0%) of them were prescribed OAC within 30 days after surgery. During follow-up (median 4.5 years, range 0‒9 years), POAF was associated with increased risk of ischemic stroke (adjusted hazard ratio [aHR] 1.18 [95% CI, 1.05‒1.32]), any thromboembolism (ischemic stroke, transient ischemic attack, or peripheral arterial embolism) (aHR 1.16, 1.05‒1.28), heart failure hospitalization (aHR 1.35, 1.21‒1.51), and recurrent atrial fibrillation (aHR 4.16, 3.76‒4.60), but not with all-cause mortality (aHR 1.08, 0.98‒1.18). Early initiation of OAC was not associated with reduced risk of ischemic stroke or any thromboembolism but with increased risk for major bleeding (aHR 1.40, 1.08‒1.82). Conclusions POAF after coronary artery bypass grafting is associated with negative prognostic impact. The role of early OAC therapy remains unclear. Studies aiming at reducing the occurrence of POAF and its consequences are warranted.
Trial registration: ClinicalTrials.gov NCT04045665.
Keywords: CABG; oral anticoagulation therapy; postoperative atrial fibrillation.
Conflict of interest statement
Jeppsson reports personal fees from Boehringer‐Ingelheim, XVIVO and LFB, outside the submitted work. Taha reports personal fees from Bayer outside the submitted work. Friberg and Bergfeldt reports personal fees from Bayer, Boehringer Ingelheim, and Sanofi, outside the submitted work. The remaining authors have no disclosures to report.
Figures


References
-
- Filardo G, Damiano RJ Jr, Ailawadi G, Thourani VH, Pollock BD, Sass DM, Phan TK, Nguyen H, da Graca B. Epidemiology of new‐onset atrial fibrillation following coronary artery bypass graft surgery. Heart. 2018;104:985–992. - PubMed
-
- Zaman AG, Archbold RA, Helft G, Paul EA, Curzen NP, Mills PG. Atrial fibrillation after coronary artery bypass surgery: a model for preoperative risk stratification. Circulation. 2000;101:1403–1408. - PubMed
-
- Anderson E, Dyke C, Levy JH. Anticoagulation strategies for the management of postoperative atrial fibrillation. Clin Lab Med. 2014;34:537–561. - PubMed
-
- Villareal RP, Hariharan R, Liu BC, Kar B, Lee VV, Elayda M, Lopez JA, Rasekh A, Wilson JM, Massumi A. Postoperative atrial fibrillation and mortality after coronary artery bypass surgery. J Am Coll Cardiol. 2004;43:742–748. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
