

White Matter Hyperintensities Are No Major Confounder for Alzheimer's Disease Cerebrospinal Fluid Biomarkers
- PMID: 33252070
- PMCID: PMC7902951
- DOI: 10.3233/JAD-200496
White Matter Hyperintensities Are No Major Confounder for Alzheimer's Disease Cerebrospinal Fluid Biomarkers
Abstract
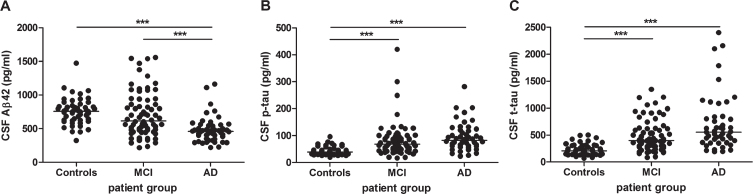
Background: The cerebrospinal fluid (CSF) biomarkers amyloid-β 1-42 (Aβ42), total and phosphorylated tau (t-tau, p-tau) are increasingly used to assist in the clinical diagnosis of Alzheimer's disease (AD). However, CSF biomarker levels can be affected by confounding factors.
Objective: To investigate the association of white matter hyperintensities (WMHs) present in the brain with AD CSF biomarker levels.
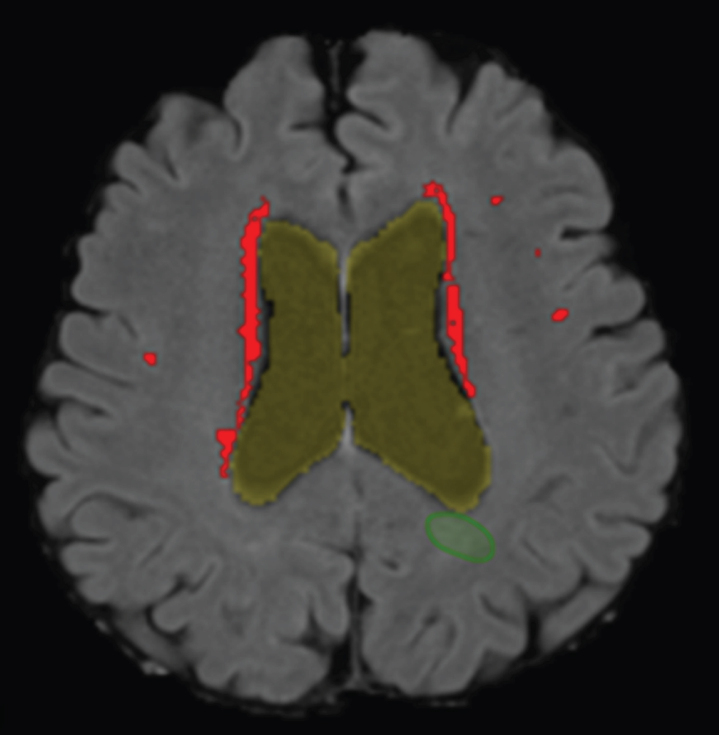
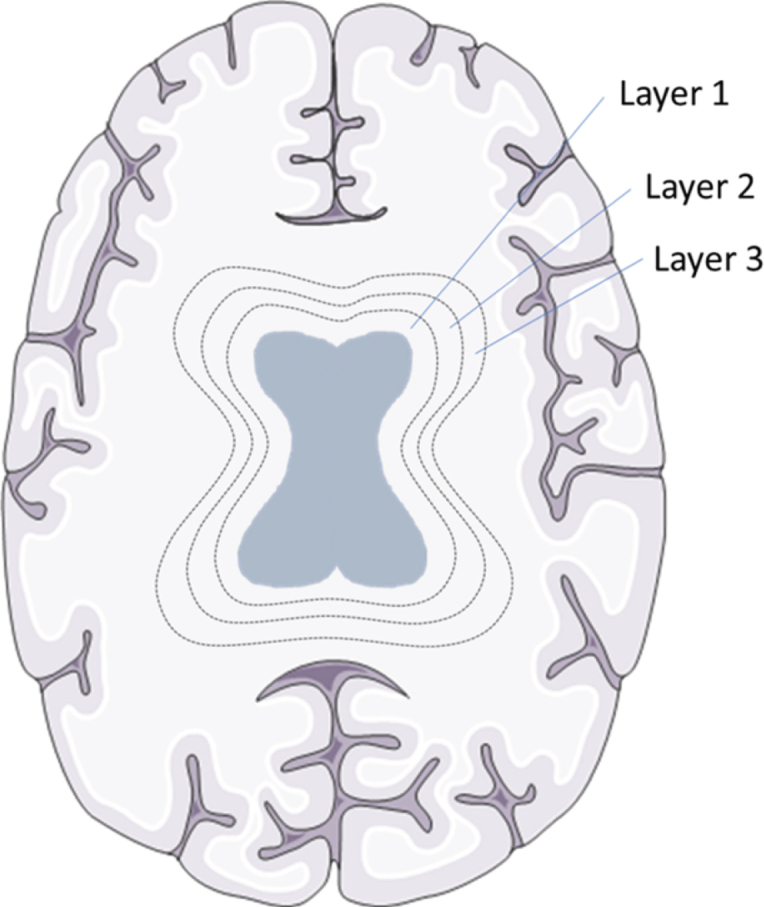
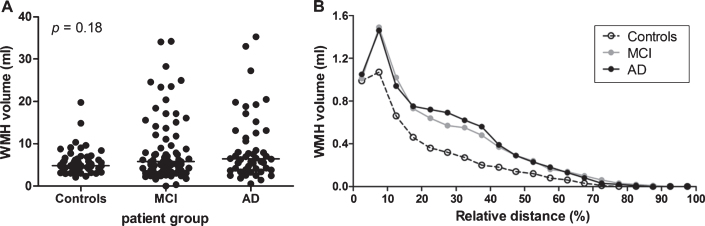
Methods: We included CSF biomarker and magnetic resonance imaging (MRI) data of 172 subjects (52 controls, 72 mild cognitive impairment (MCI), and 48 AD patients) from 9 European Memory Clinics. A computer aided detection system for standardized automated segmentation of WMHs was used on MRI scans to determine WMH volumes. Association of WMH volume with AD CSF biomarkers was determined using linear regression analysis.
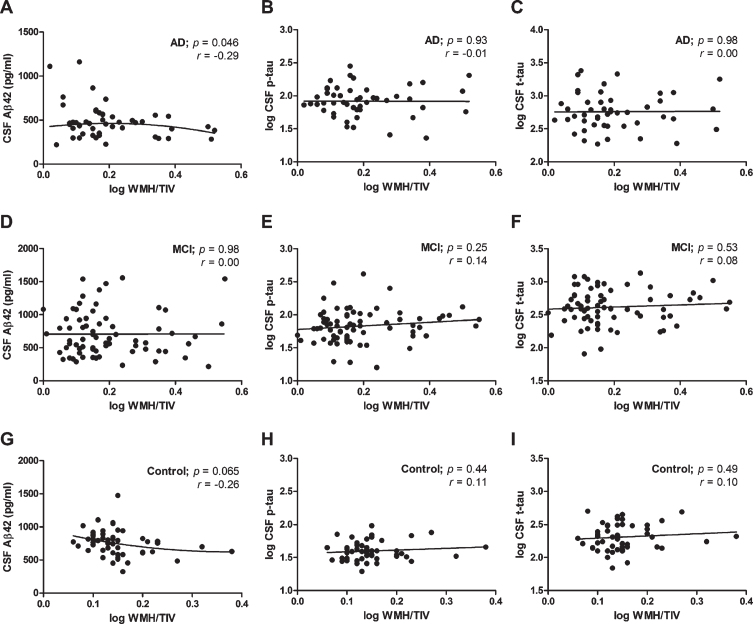
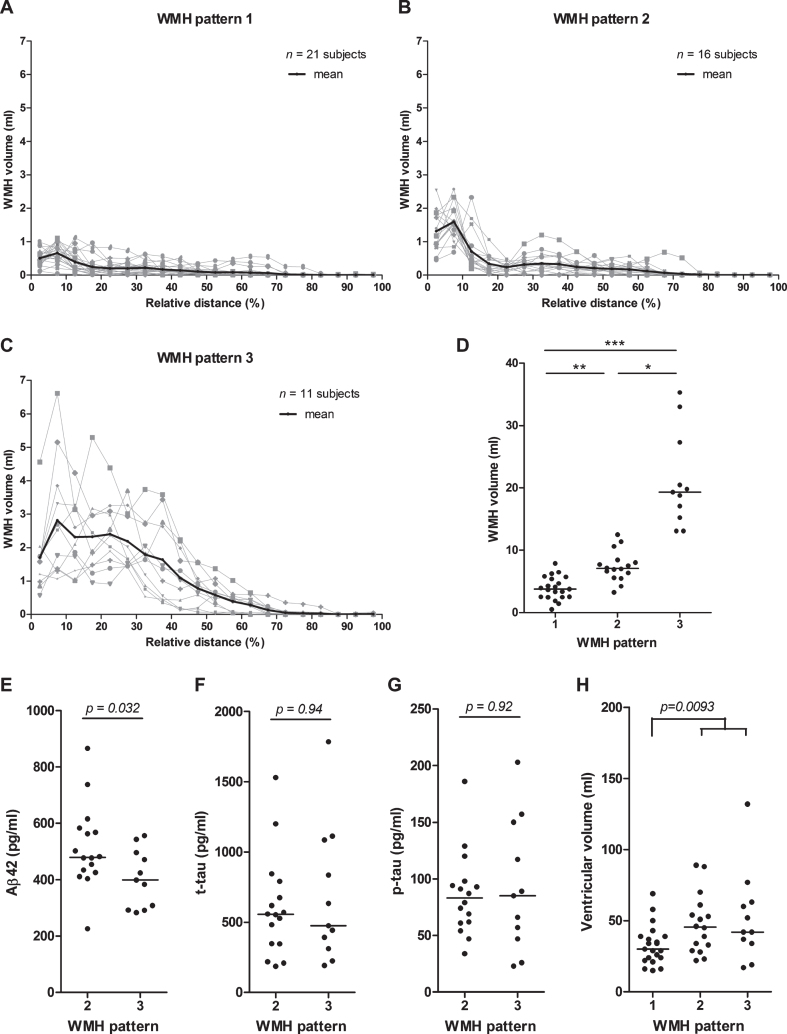
Results: A small, negative association of CSF Aβ42, but not p-tau and t-tau, levels with WMH volume was observed in the AD (r2 = 0.084, p = 0.046), but not the MCI and control groups, which was slightly increased when including the distance of WMHs to the ventricles in the analysis (r2 = 0.105, p = 0.025). Three global patterns of WMH distribution, either with 1) a low, 2) a peak close to the ventricles, or 3) a high, broadly-distributed WMH volume could be observed in brains of subjects in each diagnostic group.
Conclusion: Despite an association of WMH volume with CSF Aβ42 levels in AD patients, the occurrence of WMHs is not accompanied by excess release of cellular proteins in the CSF, suggesting that WMHs are no major confounder for AD CSF biomarker assessment.
Keywords: Alzheimer’s disease; amyloid; biomarkers; cerebrospinal fluid; magnetic resonance imaging; tau proteins; white matter hyperintensities; white matter lesions.
Conflict of interest statement
Authors’ disclosures available online (
Figures
References
-
- Blennow K, de Leon MJ, Zetterberg H (2006) Alzheimer’s disease. Lancet 368, 387–403. - PubMed
-
- Prins ND, Scheltens P (2015) White matter hyperintensities, cognitive impairment and dementia: An update. Nat Rev Neurol 11, 157–165. - PubMed
-
- Swan GE, DeCarli C, Miller BL, Reed T, Wolf PA, Jack LM, Carmelli D (1998) Association of midlife blood pressure to late-life cognitive decline and brain morphology. Neurology 51, 986–993. - PubMed
-
- Bigler ED, Kerr B, Victoroff J, Tate DF, Breitner JC (2002) White matter lesions, quantitative magnetic resonance imaging, and dementia. Alzheimer Dis Assoc Disord 16, 161–170. - PubMed
-
- De Groot JC, De Leeuw FE, Oudkerk M, Van Gijn J, Hofman A, Jolles J, Breteler MM (2002) Periventricular cerebral white matter lesions predict rate of cognitive decline. Ann Neurol 52, 335–341. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
