

Evaluation of Deep Learning to Augment Image-Guided Radiotherapy for Head and Neck and Prostate Cancers
- PMID: 33252691
- PMCID: PMC7705593
- DOI: 10.1001/jamanetworkopen.2020.27426
Evaluation of Deep Learning to Augment Image-Guided Radiotherapy for Head and Neck and Prostate Cancers
Erratum in
-
Error in Abstract.JAMA Netw Open. 2020 Dec 1;3(12):e2032624. doi: 10.1001/jamanetworkopen.2020.32624. JAMA Netw Open. 2020. PMID: 33295967 Free PMC article. No abstract available.
Abstract
Importance: Personalized radiotherapy planning depends on high-quality delineation of target tumors and surrounding organs at risk (OARs). This process puts additional time burdens on oncologists and introduces variability among both experts and institutions.
Objective: To explore clinically acceptable autocontouring solutions that can be integrated into existing workflows and used in different domains of radiotherapy.
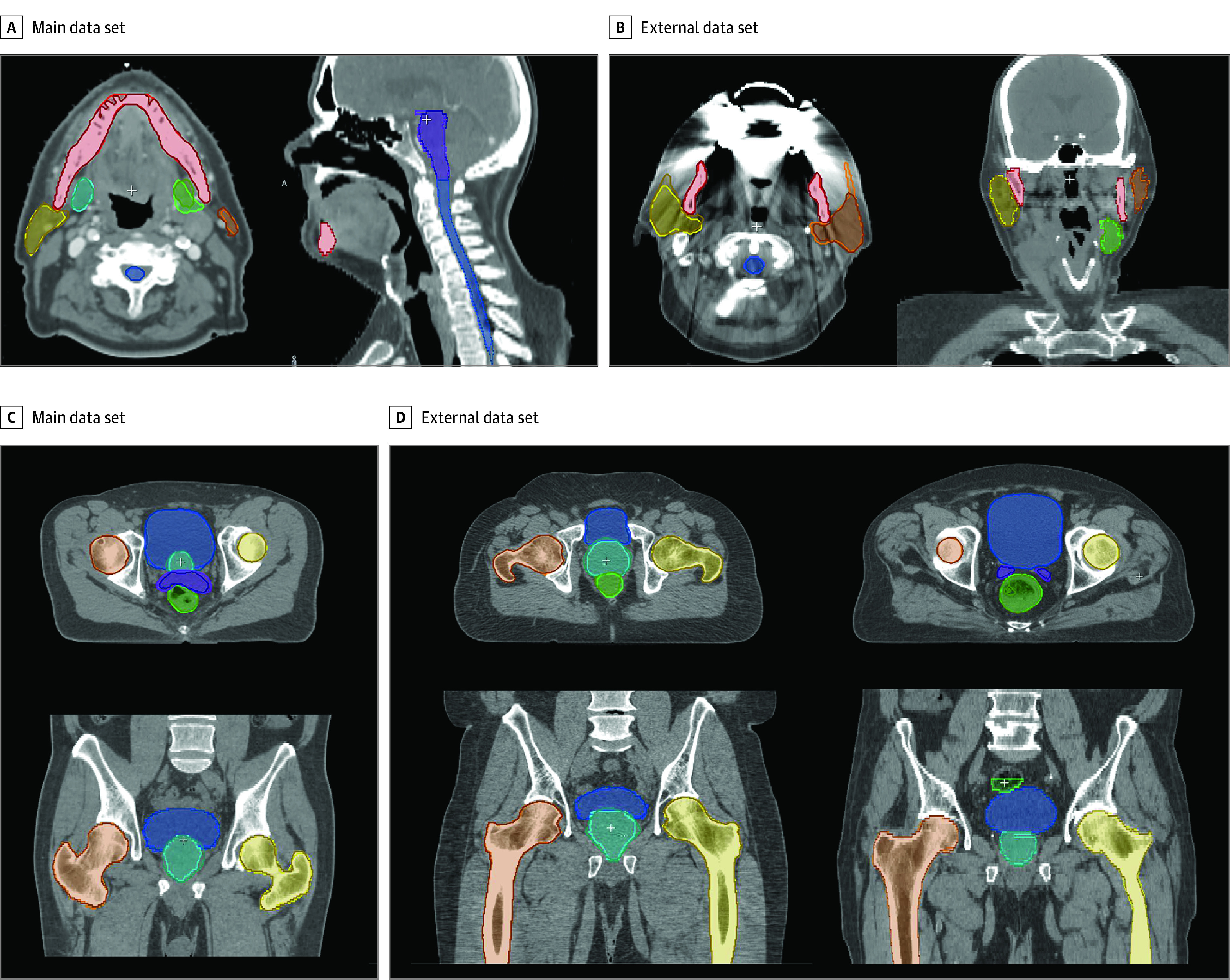
Design, setting, and participants: This quality improvement study used a multicenter imaging data set comprising 519 pelvic and 242 head and neck computed tomography (CT) scans from 8 distinct clinical sites and patients diagnosed either with prostate or head and neck cancer. The scans were acquired as part of treatment dose planning from patients who received intensity-modulated radiation therapy between October 2013 and February 2020. Fifteen different OARs were manually annotated by expert readers and radiation oncologists. The models were trained on a subset of the data set to automatically delineate OARs and evaluated on both internal and external data sets. Data analysis was conducted October 2019 to September 2020.
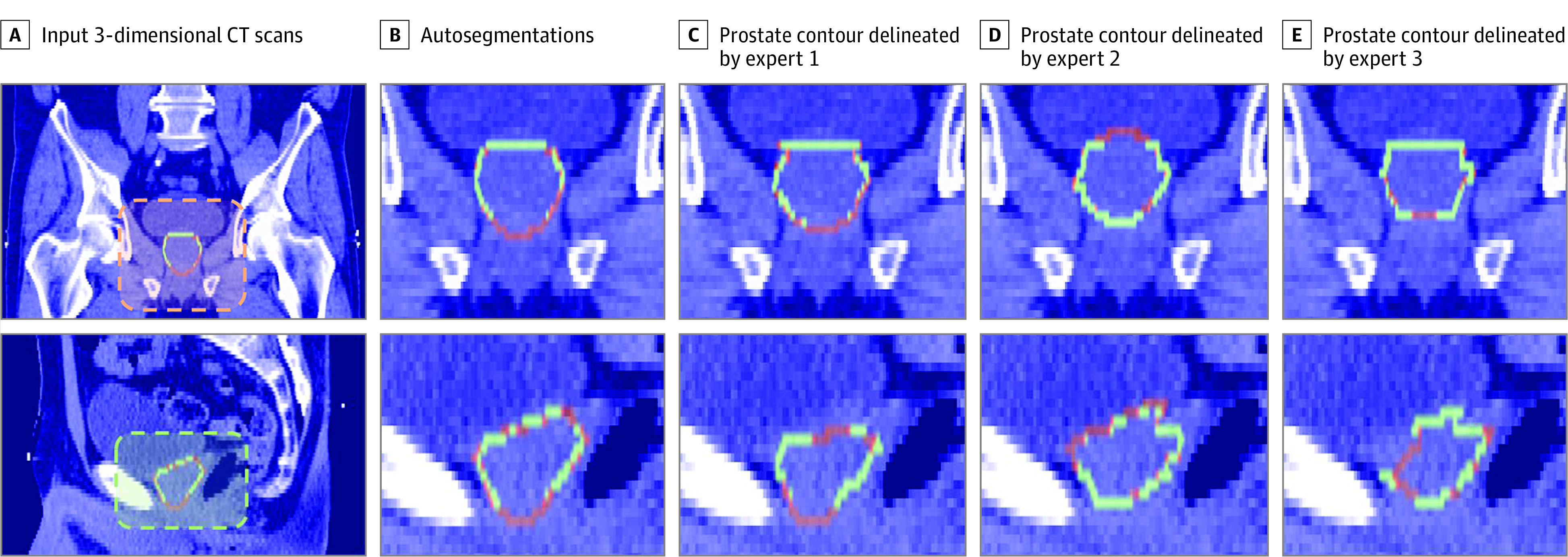
Main outcomes and measures: The autocontouring solution was evaluated on external data sets, and its accuracy was quantified with volumetric agreement and surface distance measures. Models were benchmarked against expert annotations in an interobserver variability (IOV) study. Clinical utility was evaluated by measuring time spent on manual corrections and annotations from scratch.
Results: A total of 519 participants' (519 [100%] men; 390 [75%] aged 62-75 years) pelvic CT images and 242 participants' (184 [76%] men; 194 [80%] aged 50-73 years) head and neck CT images were included. The models achieved levels of clinical accuracy within the bounds of expert IOV for 13 of 15 structures (eg, left femur, κ = 0.982; brainstem, κ = 0.806) and performed consistently well across both external and internal data sets (eg, mean [SD] Dice score for left femur, internal vs external data sets: 98.52% [0.50] vs 98.04% [1.02]; P = .04). The correction time of autogenerated contours on 10 head and neck and 10 prostate scans was measured as a mean of 4.98 (95% CI, 4.44-5.52) min/scan and 3.40 (95% CI, 1.60-5.20) min/scan, respectively, to ensure clinically accepted accuracy. Manual segmentation of the head and neck took a mean 86.75 (95% CI, 75.21-92.29) min/scan for an expert reader and 73.25 (95% CI, 68.68-77.82) min/scan for a radiation oncologist. The autogenerated contours represented a 93% reduction in time.
Conclusions and relevance: In this study, the models achieved levels of clinical accuracy within expert IOV while reducing manual contouring time and performing consistently well across previously unseen heterogeneous data sets. With the availability of open-source libraries and reliable performance, this creates significant opportunities for the transformation of radiation treatment planning.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
