

Epilepsy surveillance in normocephalic children with and without prenatal Zika virus exposure
- PMID: 33253174
- PMCID: PMC7728266
- DOI: 10.1371/journal.pntd.0008874
Epilepsy surveillance in normocephalic children with and without prenatal Zika virus exposure
Abstract
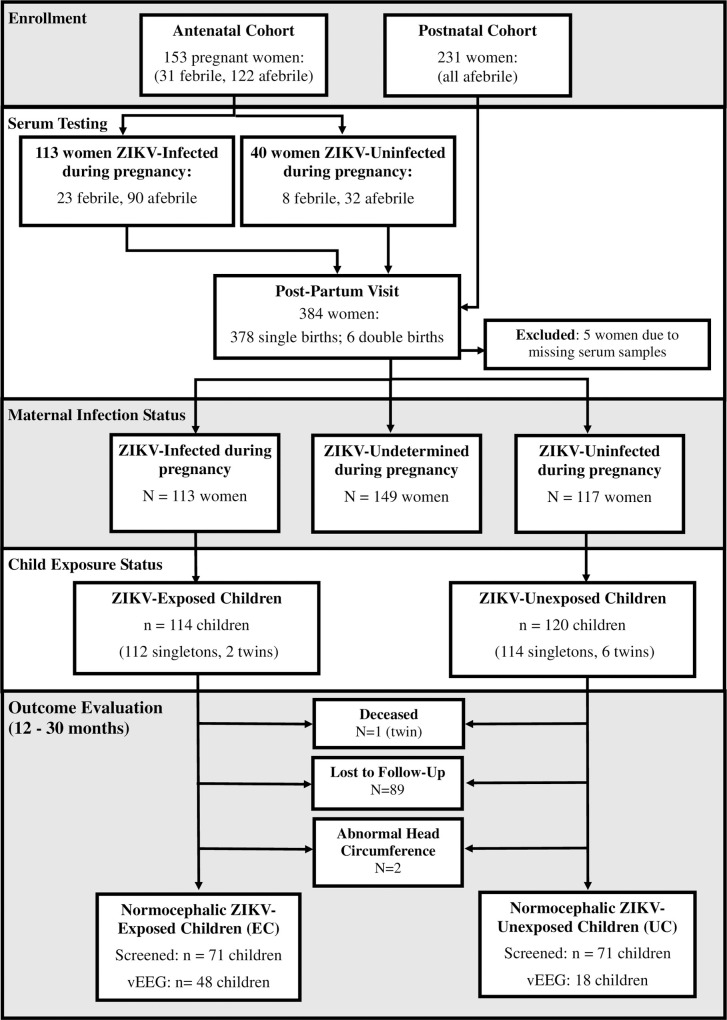
Children with Congenital Zika Syndrome and microcephaly are at high risk for epilepsy; however, the risk is unclear in normocephalic children with prenatal Zika virus (ZIKV) exposure [Exposed Children (EC)]. In this prospective cohort study, we performed epilepsy screening in normocephalic EC alongside a parallel group of normocephalic unexposed children [Unexposed Children (UC)]. We compared the incidence rate of epilepsy among EC and UC at one year of life to global incidence rates. Pregnant women were recruited from public health centers during the ZIKV outbreak in Grenada, West Indies and assessed for prior ZIKV infection using a plasmonic-gold platform that measures IgG antibodies in serum. Normocephalic children born to mothers with positive ZIKV results during pregnancy were classified as EC and those born to mothers with negative ZIKV results during and after pregnancy were classified as UC. Epilepsy screening procedures included a pediatric epilepsy screening questionnaire and video electroencephalography (vEEG). vEEG was collected using a multi-channel microEEG® system for a minimum of 20 minutes along with video recording of participant behavior time-locked to the EEG. vEEGs were interpreted independently by two pediatric epileptologists, who were blinded to ZIKV status, via telemedicine platform. Positive screening cases were referred to a local pediatrician for an epilepsy diagnostic evaluation. Epilepsy screens were positive in 2/71 EC (IR: 0.028; 95% CI: 0.003-0.098) and 0/71 UC. In both epilepsy-positive cases, questionnaire responses and interictal vEEGs were consistent with focal, rather than generalized, seizures. Both children met criteria for a clinical diagnosis of epilepsy and good seizure control was achieved with carbamazepine. Our results indicate that epilepsy rates are modestly elevated in EC. Given our small sample size, results should be considered preliminary. They support the use of epilepsy screening procedures in larger epidemiological studies of children with congenital ZIKV exposure, even in the absence of microcephaly, and provide guidance for conducting epilepsy surveillance in resource limited settings.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: Dr. Samah G. Abdel Baki reports support from Bio-Signal Group Corporation and other grants outside the submitted work. In addition, Dr. Baki has a patent 61/554,743 pending and a U.S. patent 13/284,886. None of the other authors have competing interests to disclose.
Figures

References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
