

Pain burden, sensory profile and inflammatory cytokines of dogs with naturally-occurring neuropathic pain treated with gabapentin alone or with meloxicam
- PMID: 33253197
- PMCID: PMC7703878
- DOI: 10.1371/journal.pone.0237121
Pain burden, sensory profile and inflammatory cytokines of dogs with naturally-occurring neuropathic pain treated with gabapentin alone or with meloxicam
Abstract
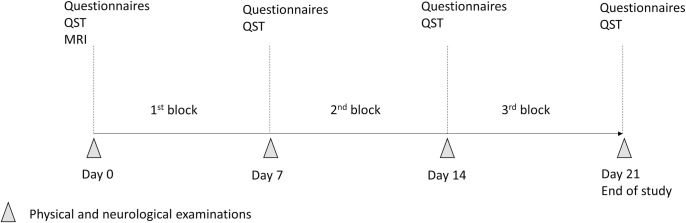
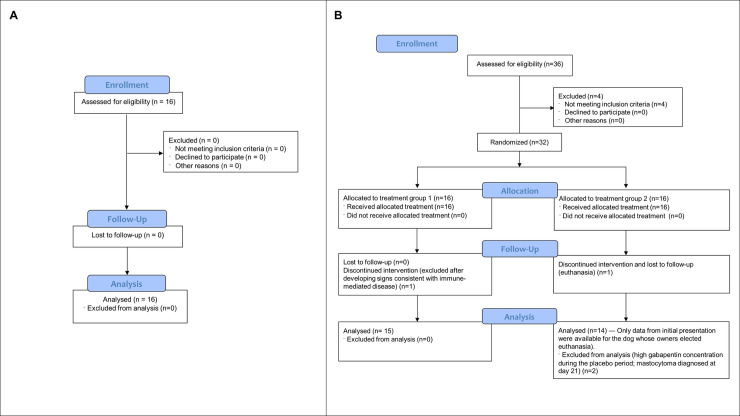
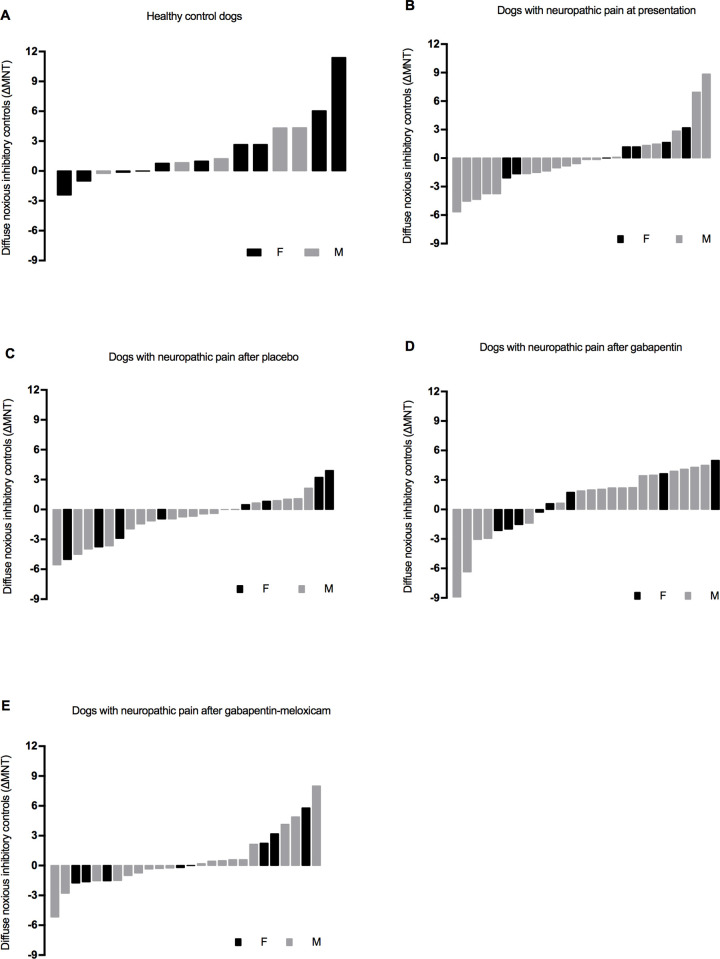
Canine neuropathic pain (NeuP) has been poorly investigated. This study aimed to evaluate the pain burden, sensory profile and inflammatory cytokines in dogs with naturally-occurring NeuP. Twenty-nine client-owned dogs with NeuP were included in a prospective, partially masked, randomized crossover clinical trial, and treated with gabapentin/placebo/gabapentin-meloxicam or gabapentin-meloxicam/placebo/gabapentin (each treatment block of 7 days; total 21 days). Pain scores, mechanical (MNT) and electrical (ENT) nociceptive thresholds and descending noxious inhibitory controls (DNIC) were assessed at baseline, days 7, 14, and 21. DNIC was evaluated using ΔMNT (after-before conditioning stimulus). Positive or negative ΔMNT corresponded to inhibitory or facilitatory pain profiles, respectively. Pain scores were recorded using the Client Specific Outcome Measures (CSOM), Canine Brief Pain Inventory (CBPI), and short-form Glasgow Composite Measure Pain Scale (CMPS-SF). Data from baseline were compared to those of sixteen healthy controls. ΔMNT, but not MNT and ENT, was significantly larger in controls (2.3 ± 0.9 N) than in NeuP (-0.2 ± 0.7 N). The percentage of dogs with facilitatory sensory profile was similar at baseline and after placebo (61.5-63%), and between controls and after gabapentin (33.3-34.6%). The CBPI scores were significantly different between gabapentin (CBPI pain and CBPI overall impression) and/or gabapentin-meloxicam (CBPI pain and interference) when compared with baseline, but not placebo. The CBPI scores were not significantly different between placebo and baseline. The concentration of cytokines was not different between groups or treatments. Dogs with NeuP have deficient inhibitory pain mechanisms. Pain burden was reduced after gabapentin and/or gabapentin-meloxicam when compared with baseline using CBPI and CMPS-SF scores. However, these scores were not superior than placebo, nor placebo was superior to baseline evaluations. A caregiver placebo effect may have biased the results.
Conflict of interest statement
This study was funded by Boehringer Ingelheim (Canada) Ltd and MITACS through the Mitacs Accelerate Program, and the American Kennel Club Canine Health Foundation. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
