

Manual Muscle Testing-Force Profiles and Their Reproducibility
- PMID: 33255648
- PMCID: PMC7759939
- DOI: 10.3390/diagnostics10120996
Manual Muscle Testing-Force Profiles and Their Reproducibility
Abstract
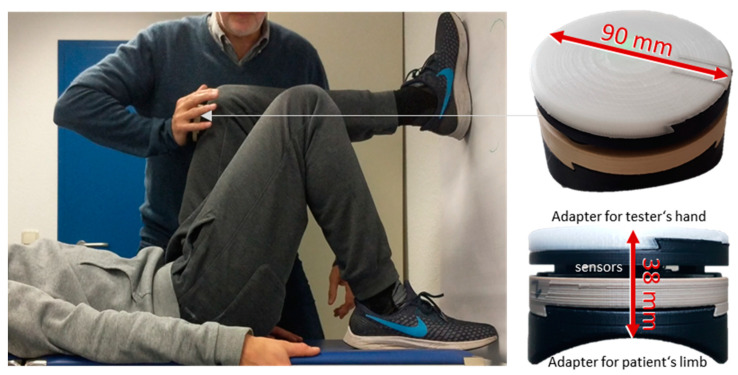
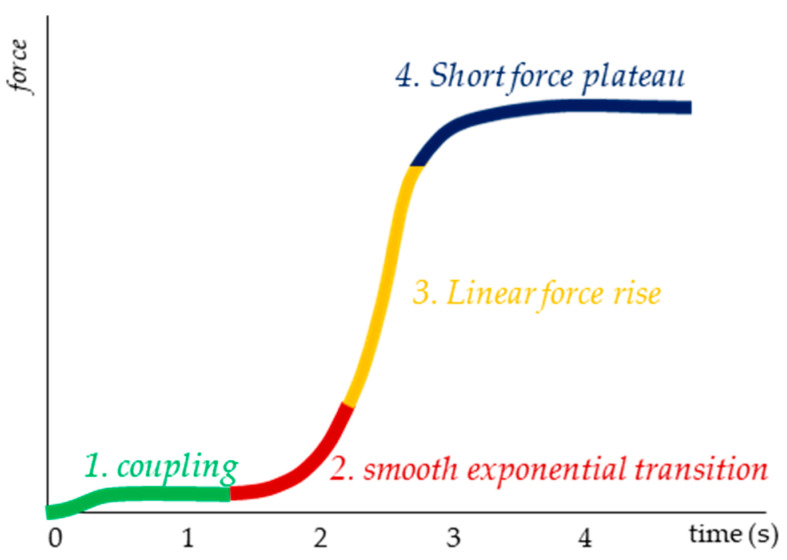
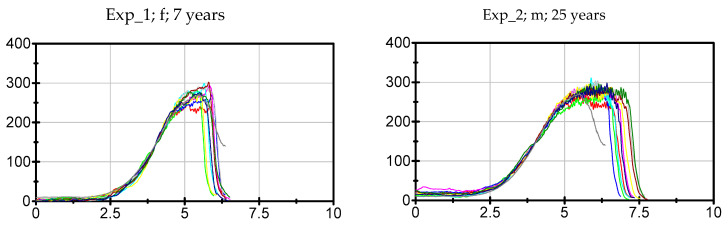
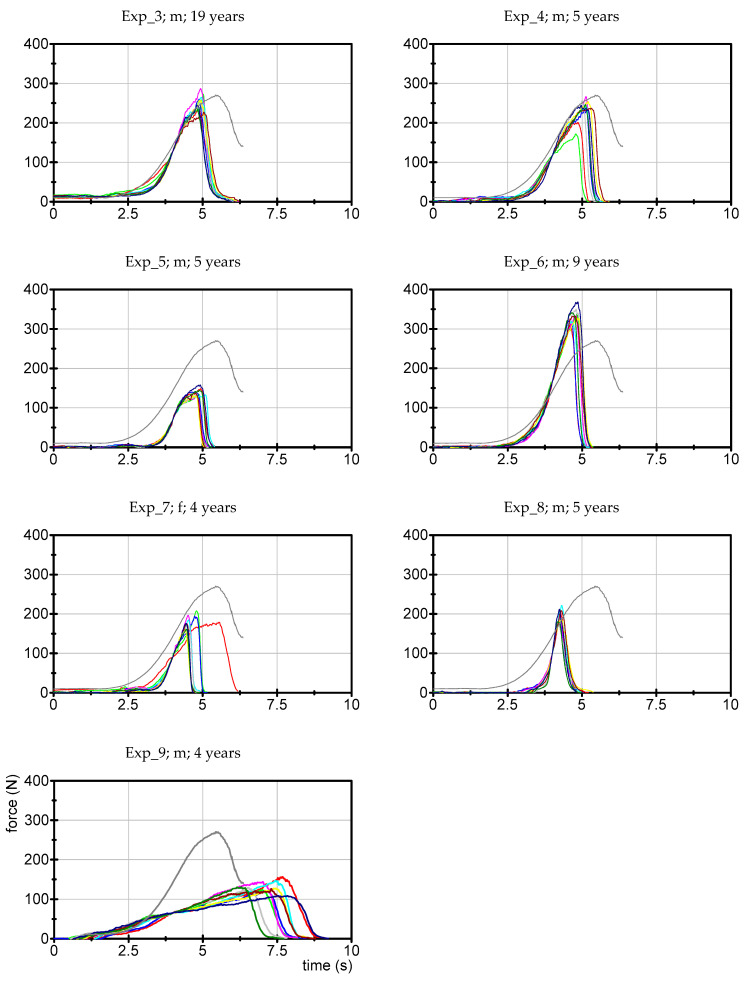
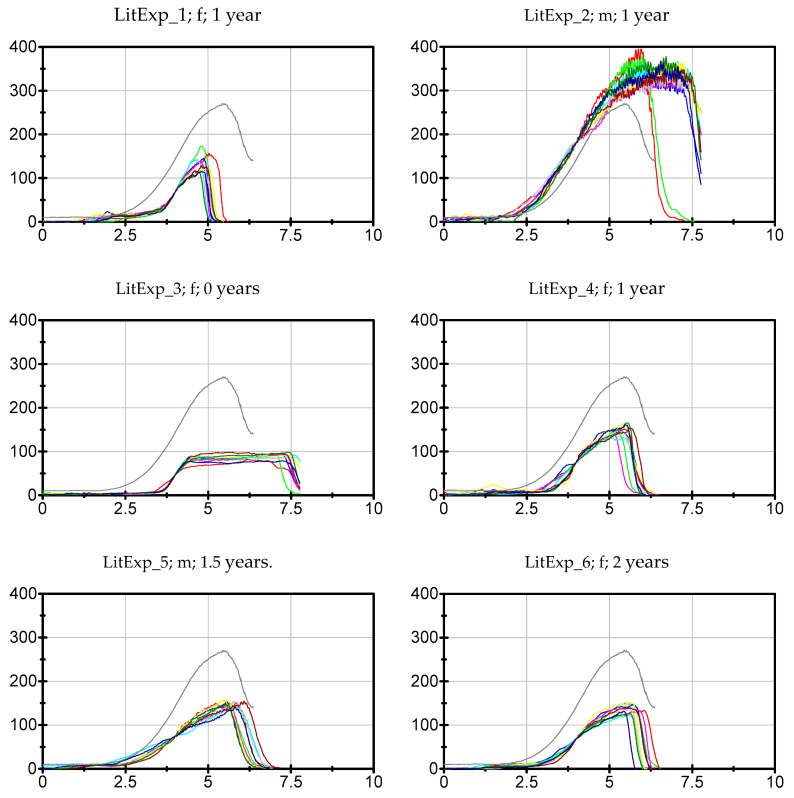
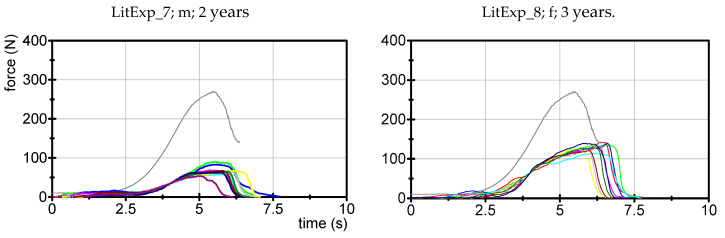
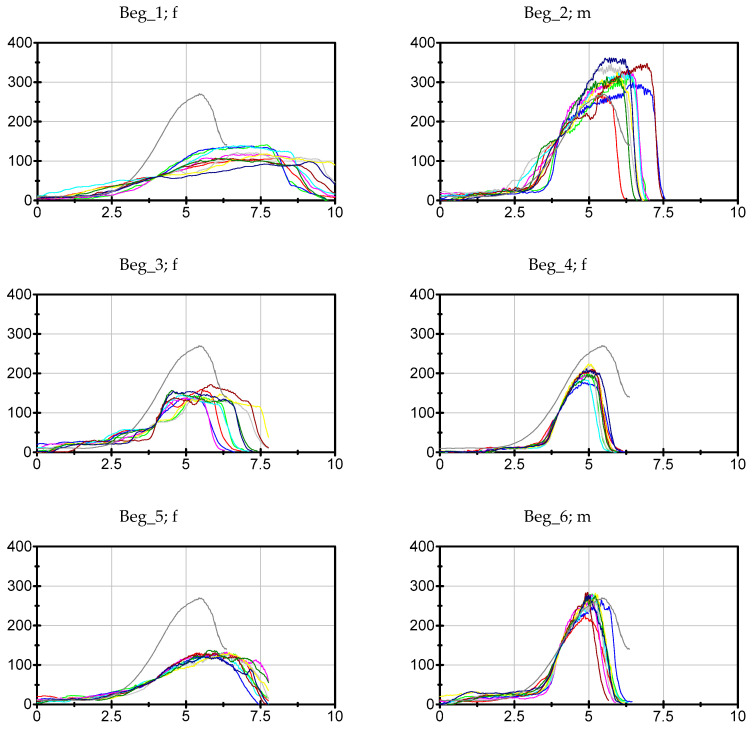
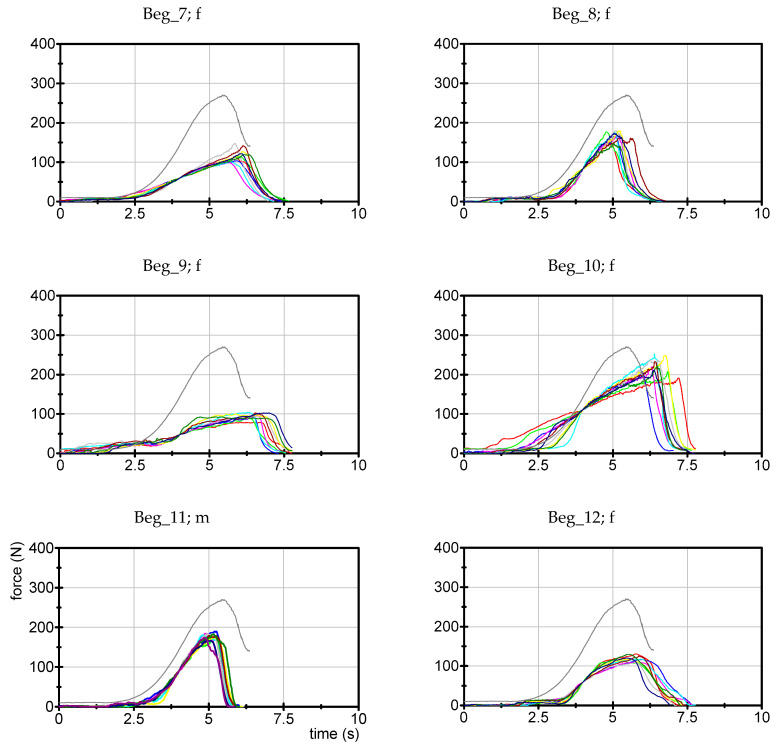
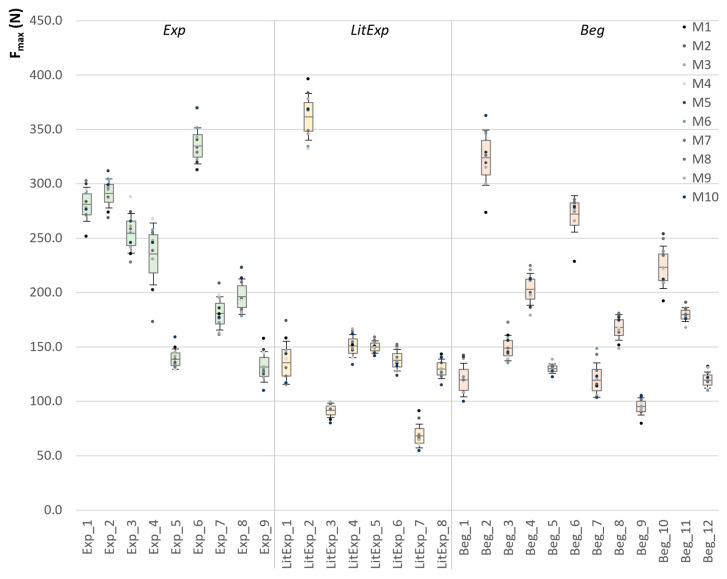
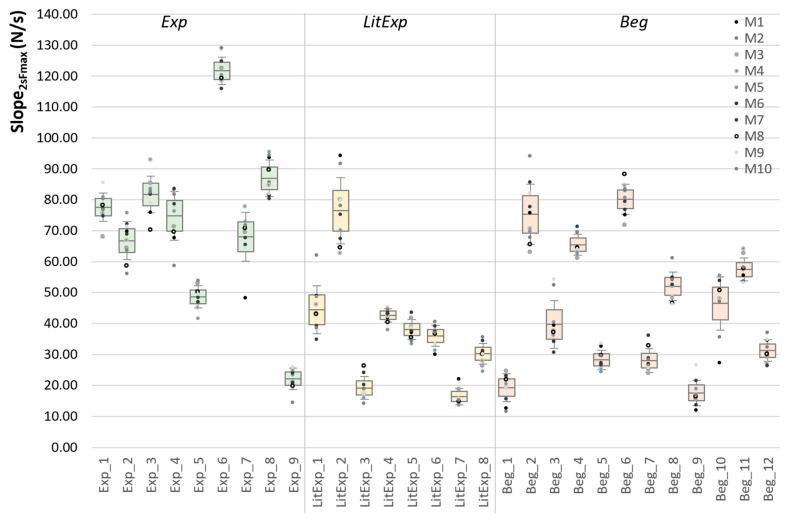
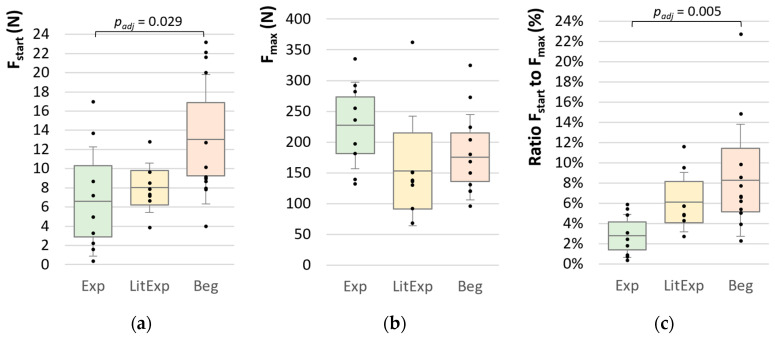
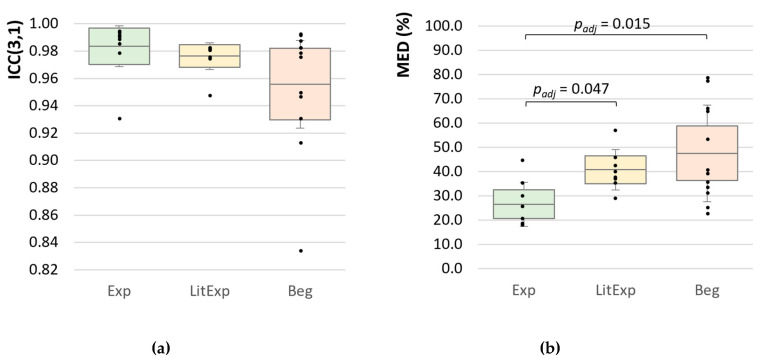
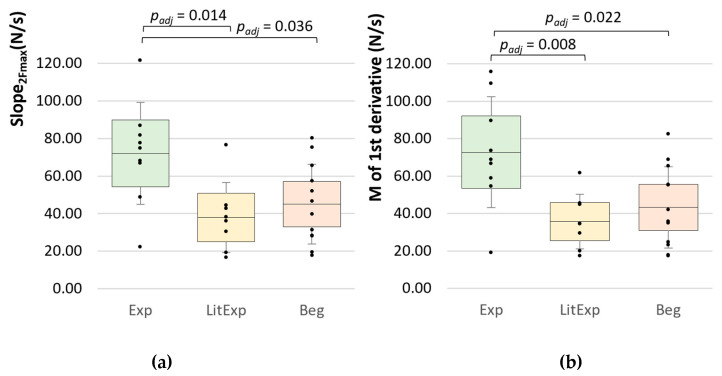
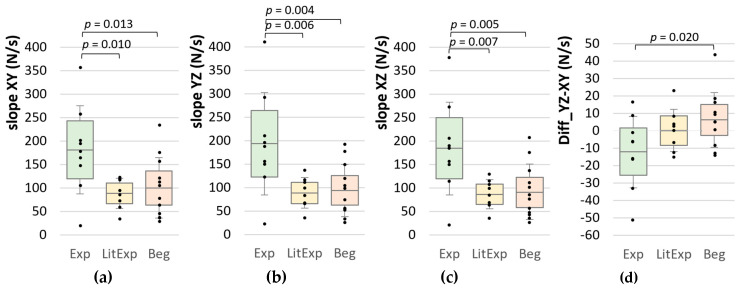
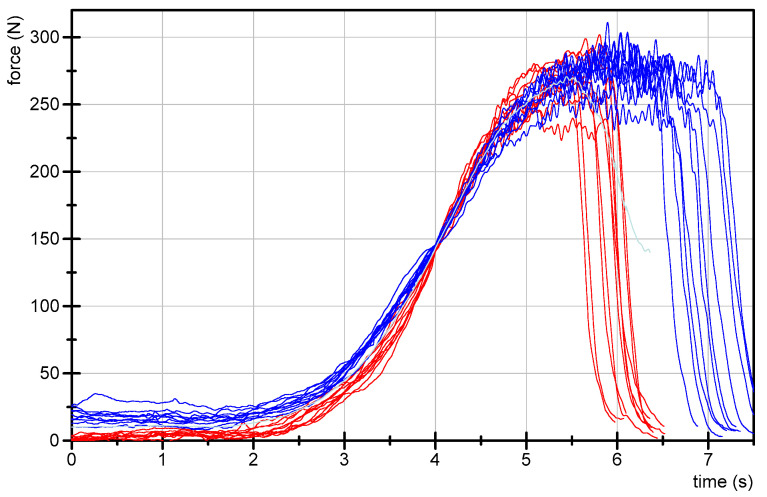
The manual muscle test (MMT) is a flexible diagnostic tool, which is used in many disciplines, applied in several ways. The main problem is the subjectivity of the test. The MMT in the version of a "break test" depends on the tester's force rise and the patient's ability to resist the applied force. As a first step, the investigation of the reproducibility of the testers' force profile is required for valid application. The study examined the force profiles of n = 29 testers (n = 9 experiences (Exp), n = 8 little experienced (LitExp), n = 12 beginners (Beg)). The testers performed 10 MMTs according to the test of hip flexors, but against a fixed leg to exclude the patient's reaction. A handheld device recorded the temporal course of the applied force. The results show significant differences between Exp and Beg concerning the starting force (padj = 0.029), the ratio of starting to maximum force (padj = 0.005) and the normalized mean Euclidean distances between the 10 trials (padj = 0.015). The slope is significantly higher in Exp vs. LitExp (p = 0.006) and Beg (p = 0.005). The results also indicate that experienced testers show inter-tester differences and partly even a low intra-tester reproducibility. This highlights the necessity of an objective MMT-assessment. Furthermore, an agreement on a standardized force profile is required. A suggestion for this is given.
Keywords: adaptive force; force profiles; handheld device; manual muscle testing; neuromuscular diagnostics; reproducibility.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Lovett R.W. The Diagnosis, Prognosis and Early Treatment of Poliomyelitis. J. Am. Med. Assoc. 1922;78:1607–1611.
-
- National Institute of Environmental Health Sciences Muscle Strength Testing—Manual Muscle Testing (MMT) [(accessed on 24 October 2020)]; Available online: https://www.niehs.nih.gov/research/resources/imacs/diseaseactivity/index....
-
- Hickie I., Davenport T., Wakefield D., Vollmer-Conna U., Cameron B., Vernon S.D., Reeves W.C., Lloyd A. Post-Infective and Chronic Fatigue Syndromes Precipitated by Viral and Non-Viral Pathogens: Prospective Cohort Study. BMJ. 2006;333:575. doi: 10.1136/bmj.38933.585764.AE. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
