

Decoding Attempted Hand Movements in Stroke Patients Using Surface Electromyography
- PMID: 33256073
- PMCID: PMC7730601
- DOI: 10.3390/s20236763
Decoding Attempted Hand Movements in Stroke Patients Using Surface Electromyography
Abstract
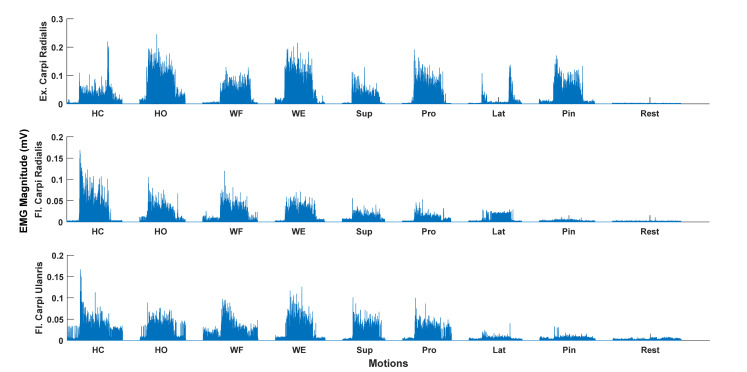
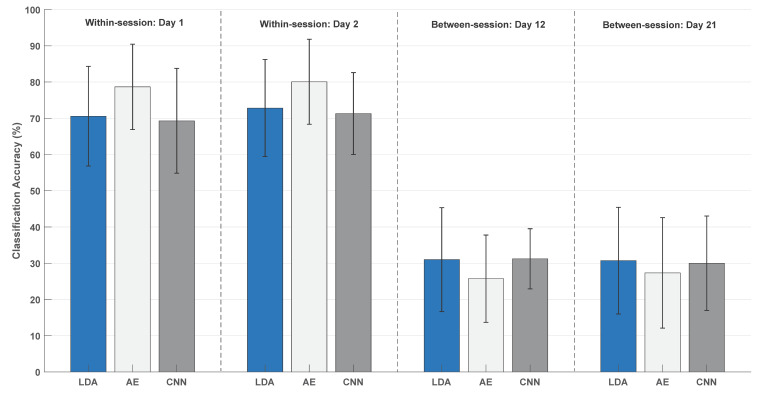
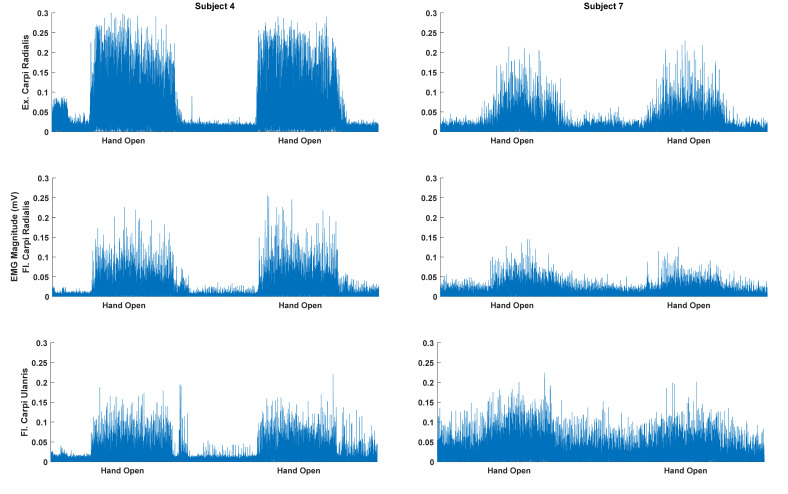
Brain- and muscle-triggered exoskeletons have been proposed as a means for motor training after a stroke. With the possibility of performing different movement types with an exoskeleton, it is possible to introduce task variability in training. It is difficult to decode different movement types simultaneously from brain activity, but it may be possible from residual muscle activity that many patients have or quickly regain. This study investigates whether nine different motion classes of the hand and forearm could be decoded from forearm EMG in 15 stroke patients. This study also evaluates the test-retest reliability of a classical, but simple, classifier (linear discriminant analysis) and advanced, but more computationally intensive, classifiers (autoencoders and convolutional neural networks). Moreover, the association between the level of motor impairment and classification accuracy was tested. Three channels of surface EMG were recorded during the following motion classes: Hand Close, Hand Open, Wrist Extension, Wrist Flexion, Supination, Pronation, Lateral Grasp, Pinch Grasp, and Rest. Six repetitions of each motion class were performed on two different days. Hudgins time-domain features were extracted and classified using linear discriminant analysis and autoencoders, and raw EMG was classified with convolutional neural networks. On average, 79 ± 12% and 80 ± 12% (autoencoders) of the movements were correctly classified for days 1 and 2, respectively, with an intraclass correlation coefficient of 0.88. No association was found between the level of motor impairment and classification accuracy (Spearman correlation: 0.24). It was shown that nine motion classes could be decoded from residual EMG, with autoencoders being the best classification approach, and that the results were reliable across days; this may have implications for the development of EMG-controlled exoskeletons for training in the patient's home.
Keywords: EMG; brain-computer interface; myoelectric control; pattern recognition; stroke.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Decoding of Ankle Joint Movements in Stroke Patients Using Surface Electromyography.Sensors (Basel). 2021 Feb 24;21(5):1575. doi: 10.3390/s21051575. Sensors (Basel). 2021. PMID: 33668229 Free PMC article.
-
Comparison of EEG measurement of upper limb movement in motor imagery training system.Biomed Eng Online. 2018 Aug 2;17(1):103. doi: 10.1186/s12938-018-0534-0. Biomed Eng Online. 2018. PMID: 30071853 Free PMC article.
-
Resolving the effect of wrist position on myoelectric pattern recognition control.J Neuroeng Rehabil. 2017 May 4;14(1):39. doi: 10.1186/s12984-017-0246-x. J Neuroeng Rehabil. 2017. PMID: 28472991 Free PMC article.
-
Artificial neural network EMG classifier for functional hand grasp movements prediction.J Int Med Res. 2017 Dec;45(6):1831-1847. doi: 10.1177/0300060516656689. Epub 2016 Sep 27. J Int Med Res. 2017. PMID: 27677300 Free PMC article.
-
Comparison of surface and intramuscular EMG pattern recognition for simultaneous wrist/hand motion classification.Annu Int Conf IEEE Eng Med Biol Soc. 2013;2013:4223-6. doi: 10.1109/EMBC.2013.6610477. Annu Int Conf IEEE Eng Med Biol Soc. 2013. PMID: 24110664 Free PMC article.
Cited by
-
Empirical Myoelectric Feature Extraction and Pattern Recognition in Hemiplegic Distal Movement Decoding.Bioengineering (Basel). 2023 Jul 21;10(7):866. doi: 10.3390/bioengineering10070866. Bioengineering (Basel). 2023. PMID: 37508895 Free PMC article.
-
Facial EMG Activity Is Associated with Hedonic Experiences but not Nutritional Values While Viewing Food Images.Nutrients. 2020 Dec 22;13(1):11. doi: 10.3390/nu13010011. Nutrients. 2020. PMID: 33375209 Free PMC article.
-
Optimizing the impact of time domain segmentation techniques on upper limb EMG decoding using multimodal features.PLoS One. 2025 May 8;20(5):e0322580. doi: 10.1371/journal.pone.0322580. eCollection 2025. PLoS One. 2025. PMID: 40338888 Free PMC article.
-
Supervised Myoelectrical Hand Gesture Recognition in Post-Acute Stroke Patients with Upper Limb Paresis on Affected and Non-Affected Sides.Sensors (Basel). 2022 Nov 11;22(22):8733. doi: 10.3390/s22228733. Sensors (Basel). 2022. PMID: 36433330 Free PMC article.
-
Decoding of Ankle Joint Movements in Stroke Patients Using Surface Electromyography.Sensors (Basel). 2021 Feb 24;21(5):1575. doi: 10.3390/s21051575. Sensors (Basel). 2021. PMID: 33668229 Free PMC article.
References
-
- Krakauer J.W. Motor learning: Its relevance to stroke recovery and neurorehabilitation. Curr. Opin. Neurol. 2006;19:84–90. doi: 10.1097/01.wco.0000200544.29915.cc. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
