

Boerhaave syndrome due to excessive alcohol consumption: two case reports
- PMID: 33256613
- PMCID: PMC7706278
- DOI: 10.1186/s12245-020-00318-5
Boerhaave syndrome due to excessive alcohol consumption: two case reports
Abstract
Background: Spontaneous esophageal rupture, or Boerhaave syndrome, is a fatal disorder caused by an elevated esophageal pressure owing to forceful vomiting. Patients with Boerhaave syndrome often present with chest pain, dyspnea, and shock. We report on two patients of Boerhaave syndrome with different severities that was triggered by excessive alcohol consumption and was diagnosed immediately in the emergency room.
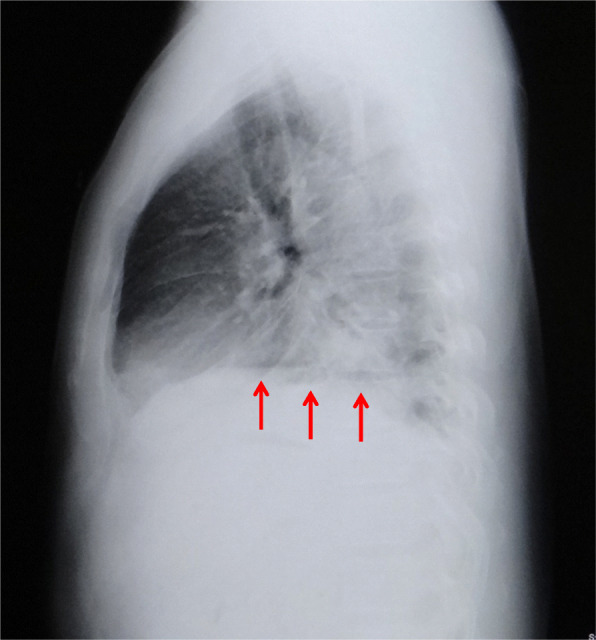
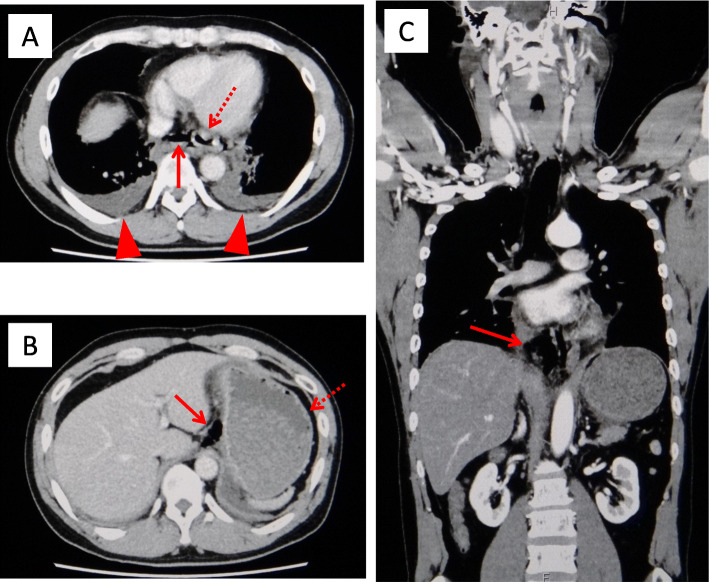
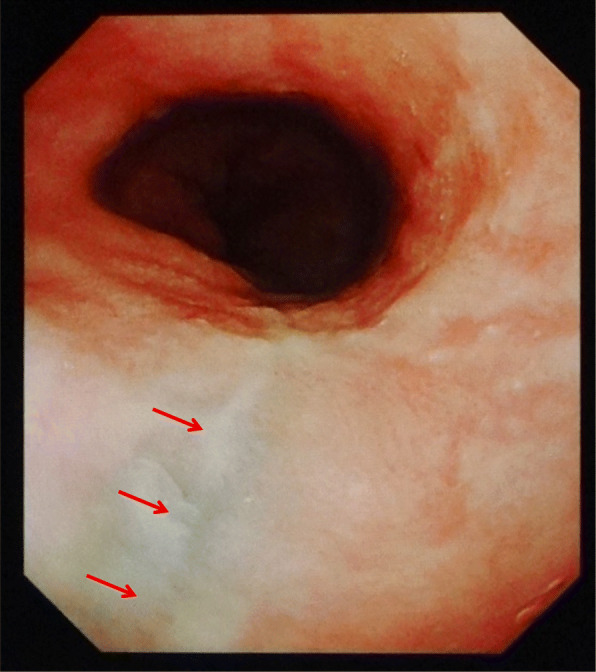
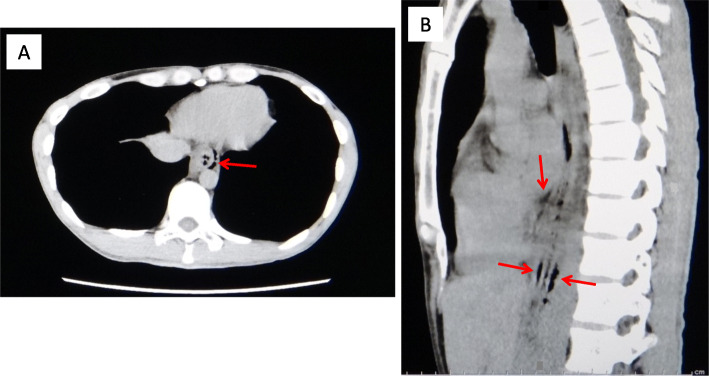
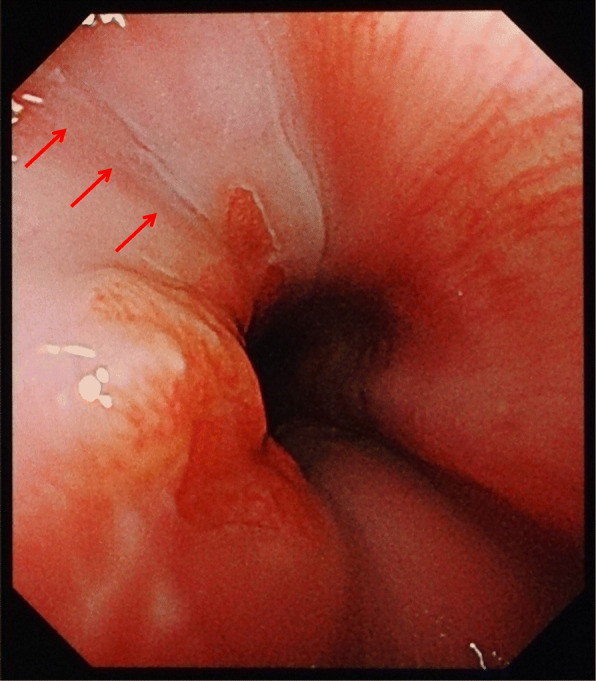
Case presentation: The patient in case 1 complained of severe chest pain and nausea and vomited on arrival at the hospital. He was subsequently diagnosed with Boerhaave syndrome coupled with mediastinitis using computed tomography (CT) and esophagogram. An emergency operation was successfully performed, in which a 3-cm tear was found on the left posterior wall of the distal esophagus. The patient subsequently had anastomotic leakage but was discharged 41 days later. The patient in case 2 complained of severe chest pain, nausea, vomiting, and hematemesis on arrival. He was suggested of having Boerhaave syndrome without mediastinitis on CT. The symptoms gradually disappeared after conservative treatment. Upper gastrointestinal endoscopy performed on the ninth day revealed a scar on the left wall of the distal esophagus. The patient was discharged 11 days later. In addition to the varying severity between the cases, the patient in case 2 was initially considered to have Mallory-Weiss syndrome.
Conclusion: Owing to similar histories and symptoms, Boerhaave syndrome and Mallory-Weiss syndrome must be accurately distinguished by emergency clinicians. CT can be a useful modality to detect any severity of Boerhaave syndrome and also offers the possibility to distinguish Boerhaave syndrome from Mallory-Weiss syndrome.
Keywords: Boerhaave syndrome; Chest pain; Hematemesis; Mallory–Weiss syndrome; Vomiting.
Conflict of interest statement
The authors declare that they have no competing interests. This manuscript has not been published and is not under consideration for publication elsewhere. Additionally, all of the authors have approved the contents of this paper and have agreed to the journal’s submission policies.
Figures
References
-
- Turner AR, Turner SD. Boerhaave syndrome. StatPearls Publ. 2020. https://www.ncbi.nlm.nih.gov/books/NBK430808/. Accessed 25 July 2020.
-
- Mackler SA. Spontaneous rupture of the esophagus. An experimental and clinical study. Surg Gynecol Obestet. 1952;95:345–356. - PubMed
LinkOut - more resources
Full Text Sources
