

Right ventricular-arterial uncoupling independently predicts survival in COVID-19 ARDS
- PMID: 33256813
- PMCID: PMC7703719
- DOI: 10.1186/s13054-020-03385-5
Right ventricular-arterial uncoupling independently predicts survival in COVID-19 ARDS
Abstract
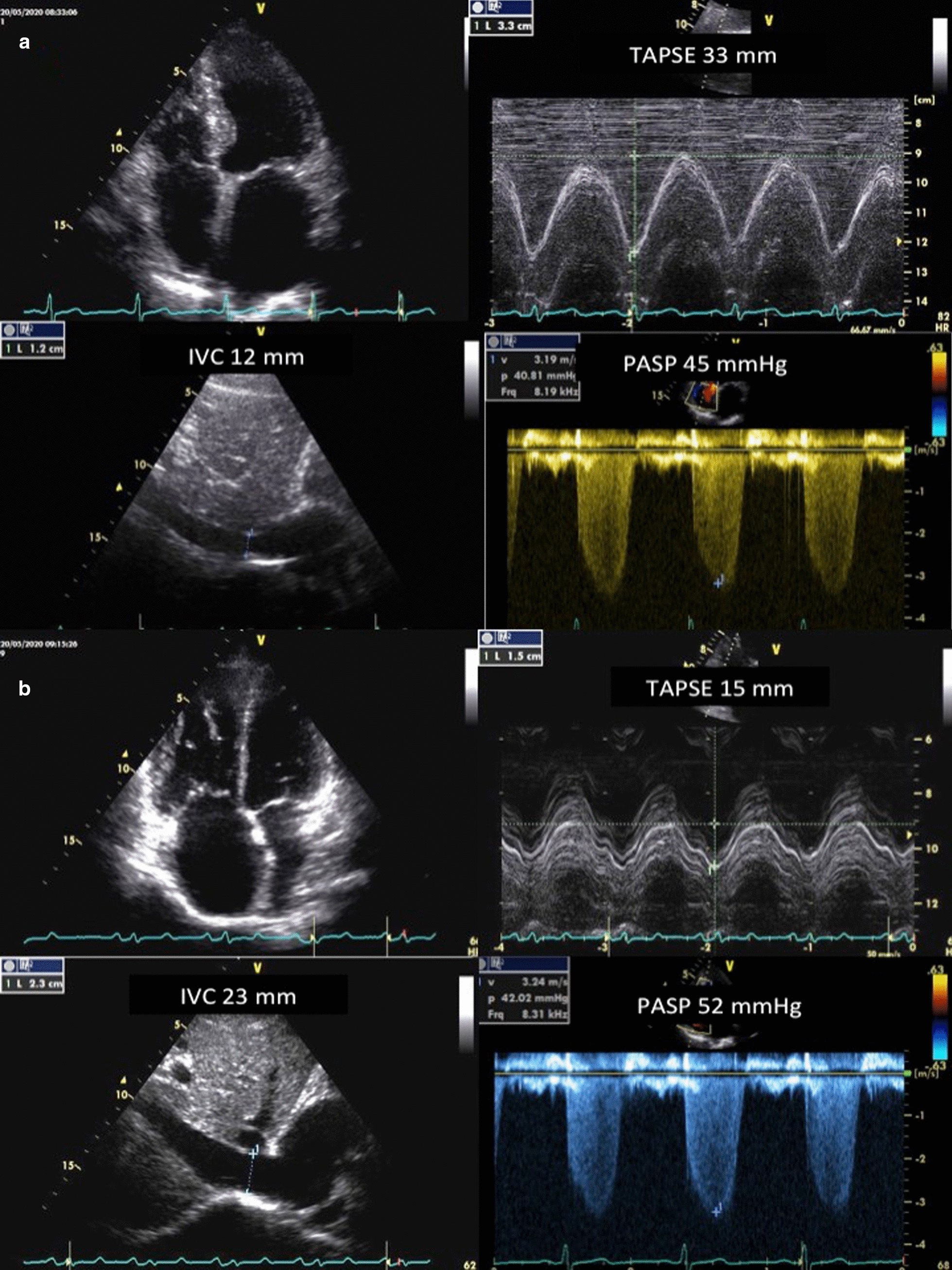
Aim: To investigate the prevalence and prognostic impact of right heart failure and right ventricular-arterial uncoupling in Corona Virus Infectious Disease 2019 (COVID-19) complicated by an Acute Respiratory Distress Syndrome (ARDS).
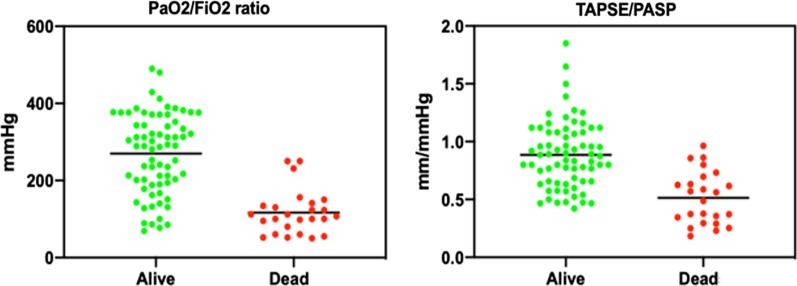
Methods: Ninety-four consecutive patients (mean age 64 years) admitted for acute respiratory failure on COVID-19 were enrolled. Coupling of right ventricular function to the pulmonary circulation was evaluated by a comprehensive trans-thoracic echocardiography with focus on the tricuspid annular plane systolic excursion (TAPSE) to systolic pulmonary artery pressure (PASP) ratio RESULTS: The majority of patients needed ventilatory support, which was noninvasive in 22 and invasive in 37. There were 25 deaths, all in the invasively ventilated patients. Survivors were younger (62 ± 13 vs. 68 ± 12 years, p = 0.033), less often overweight or usual smokers, had lower NT-proBNP and interleukin-6, and higher arterial partial pressure of oxygen (PaO2)/fraction of inspired O2 (FIO2) ratio (270 ± 104 vs. 117 ± 57 mmHg, p < 0.001). In the non-survivors, PASP was increased (42 ± 12 vs. 30 ± 7 mmHg, p < 0.001), while TAPSE was decreased (19 ± 4 vs. 25 ± 4 mm, p < 0.001). Accordingly, the TAPSE/PASP ratio was lower than in the survivors (0.51 ± 0.22 vs. 0.89 ± 0.29 mm/mmHg, p < 0.001). At univariate/multivariable analysis, the TAPSE/PASP (HR: 0.026; 95%CI 0.01-0.579; p: 0.019) and PaO2/FIO2 (HR: 0.988; 95%CI 0.988-0.998; p: 0.018) ratios were the only independent predictors of mortality, with ROC-determined cutoff values of 159 mmHg and 0.635 mm/mmHg, respectively.
Conclusions: COVID-19 ARDS is associated with clinically relevant uncoupling of right ventricular function from the pulmonary circulation; bedside echocardiography of TAPSE/PASP adds to the prognostic relevance of PaO2/FIO2 in ARDS on COVID-19.
Keywords: ARDS; COVID-19; Echocardiography; Prognosis; Right ventricular-arterial uncoupling.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, Cereda D, Coluccello A, Foti G, Fumagalli R, Iotti G, Latronico N, Lorini L, Merler S, Natalini G, Piatti A, Ranieri MV, Scandroglio AM, Storti E, Cecconi M, Pesenti M. COVID-19 lombardy ICU network. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA. 2020;323:1574–1581. doi: 10.1001/jama.2020.5394. - DOI - PMC - PubMed
-
- Bhatraju PK, Ghassemieh BJ, Nichols M, Kim R, Jerome KR, Nalla AK, Greninger AL, Pipavath S, Wurfel MM, Evans L, Kritek PA, West TE, Luks A, Gerbino A, Dale CR, Goldman JD, O'Mahony S, Mikacenic C. Covid-19 in critically Ill patients in the Seattle region—case series. N Engl J Med. 2020;382:2012–2022. doi: 10.1056/NEJMoa2004500. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
