

Ultrasonography-guided closed reduction in the treatment of displaced transphyseal fracture of the distal humerus
- PMID: 33256817
- PMCID: PMC7708137
- DOI: 10.1186/s13018-020-02118-2
Ultrasonography-guided closed reduction in the treatment of displaced transphyseal fracture of the distal humerus
Abstract
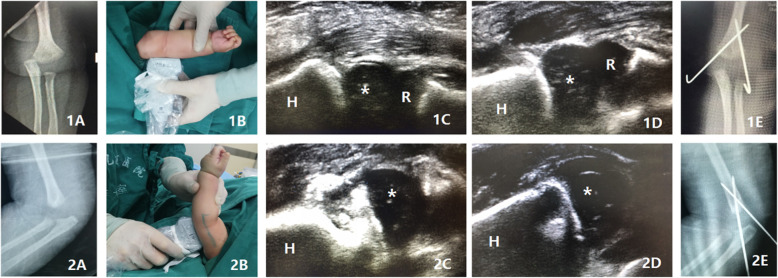
Background: To evaluate the clinical and radiographic outcomes of ultrasonography-guided closed reduction in the treatment of displaced transphyseal fracture of the distal humerus (TFDH).
Methods: Twenty-seven patients with displaced TFDH were successfully treated by the ultrasonography-guided closed reduction during January 2012 to December 2016 and were retrospectively reviewed. After the mean follow-up of 34.88 months, the clinical and radiographic outcomes of patients were evaluated. The cubitus varus of the affected elbows was also assessed at the latest follow-up.
Results: The successful rate of ultrasonography-guided closed reduction in the treatment of displaced TFDH was 84% (27/32). The twenty-seven patients with successful reduction were included for the following analysis. There were 20 males and 7 females included in the study, and the mean age at treatment was 15.39 ± 3.10 months; seventeen fractures occurred in the right side elbow and ten in the left side. At the last follow-up, there were significant decreases in the elbow flexion (3°, P = 0.027) and range of motion (5°, P = 0.003) between the injured and uninjured elbow, respectively, whereas no difference in elbow extension was detected (P = 0.110). Flynn's criteria assessment showed that all the patients achieved excellent or good outcomes both in the functional and cosmetic categories. The clinical and radiographic carrying angles at the last follow-up were 11.67 ± 3.11° and 10.46 ± 3.88°, respectively. And the incidence of cubitus varus after treatment was 7.4% at the last follow-up.
Conclusion: The ultrasonography-guided closed reduction in the treatment of displaced TFDH is an effective procedure; the adequate fracture reduction can be acquired with the advantages of real-time, non-radioactive, and simple utilization. With the percutaneous pining fixation, satisfactory clinical and radiographic outcomes can be achieved with a low incidence of postoperative cubitus varus.
Keywords: Closed reduction; Displaced transphyseal fracture of the distal humerus; Ultrasonography.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
[Ultrasound-guided reduction and percutaneous crossed pin fixation for the treatment of displaced supracondylar fracture of the humerus in children].Zhongguo Gu Shang. 2020 Oct 25;33(10):907-11. doi: 10.12200/j.issn.1003-0034.2020.10.004. Zhongguo Gu Shang. 2020. PMID: 33107251 Chinese.
-
Radiologic, clinical, and functional evaluation of children with displaced T-condylar fractures treated by closed reduction and percutaneous fixation using the Mayo Elbow Performance Score.Int Orthop. 2024 Jun;48(6):1471-1479. doi: 10.1007/s00264-023-06058-4. Epub 2023 Dec 20. Int Orthop. 2024. PMID: 38117292
-
[Lateral closing wedge osteotomy for treatment of traumatic cubitus varus deformity in children].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2012 Jun;26(6):657-60. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2012. PMID: 22792757 Chinese.
-
Transphyseal elbow fracture in newborn: review of literature.Musculoskelet Surg. 2015 Sep;99 Suppl 1:S99-105. doi: 10.1007/s12306-015-0366-z. Epub 2015 May 10. Musculoskelet Surg. 2015. PMID: 25957551 Review.
-
Management of lateral humeral condylar fracture in children.J Am Acad Orthop Surg. 2011 Jun;19(6):350-8. doi: 10.5435/00124635-201106000-00005. J Am Acad Orthop Surg. 2011. PMID: 21628646 Review.
Cited by
-
Application of ultrasound in the closed reduction and percutaneous pinning in supracondylar humeral fractures.J Orthop Surg Res. 2021 Oct 12;16(1):588. doi: 10.1186/s13018-021-02755-1. J Orthop Surg Res. 2021. PMID: 34641943 Free PMC article.
-
Closed Reduction and Percutaneous Pinning in the Treatment of Humeral Distal Metaphyseal-Diaphyseal Junction Fractures in Children: A Technique Note and Preliminary Results.Front Pediatr. 2021 Jun 17;9:670164. doi: 10.3389/fped.2021.670164. eCollection 2021. Front Pediatr. 2021. PMID: 34222144 Free PMC article.
-
The emerging application of ultrasound technology in pediatric bone fractures: Clinical application, related issues and development prospect.Pediatr Discov. 2024 May 28;2(2):e69. doi: 10.1002/pdi3.69. eCollection 2024 Jun. Pediatr Discov. 2024. PMID: 40625891 Free PMC article. Review.
-
Comparative use of ultrasound and radiography for the detection of fractures: a systematic review and narrative synthesis.Ann Med Surg (Lond). 2023 Sep 5;85(10):5085-5095. doi: 10.1097/MS9.0000000000001229. eCollection 2023 Oct. Ann Med Surg (Lond). 2023. PMID: 37811018 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
