

Lung transplantation for patients with severe COVID-19
- PMID: 33257409
- PMCID: PMC8050952
- DOI: 10.1126/scitranslmed.abe4282
Lung transplantation for patients with severe COVID-19
Abstract
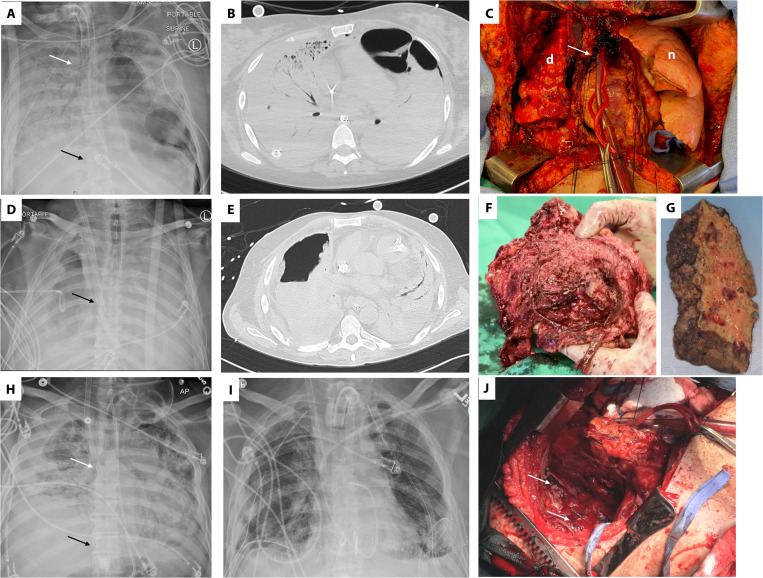
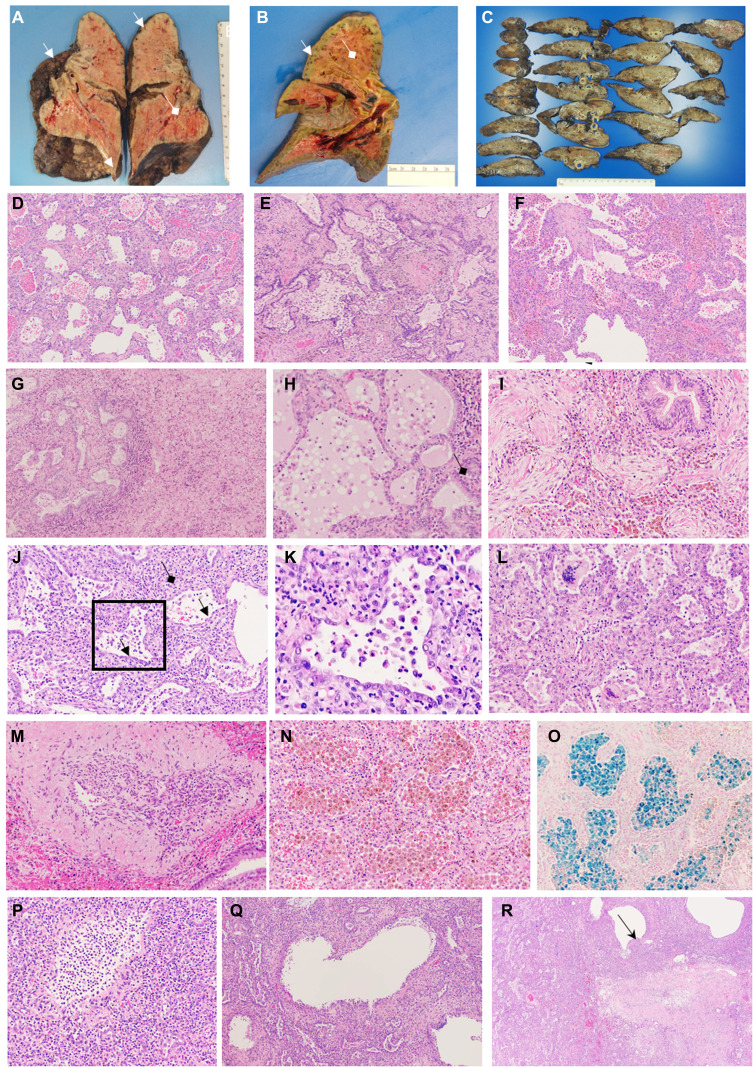
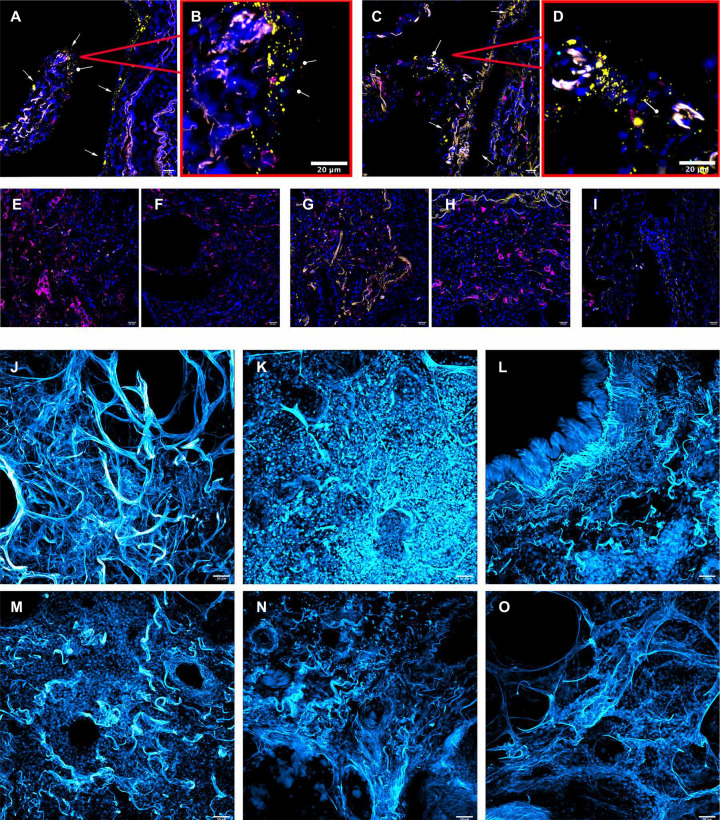
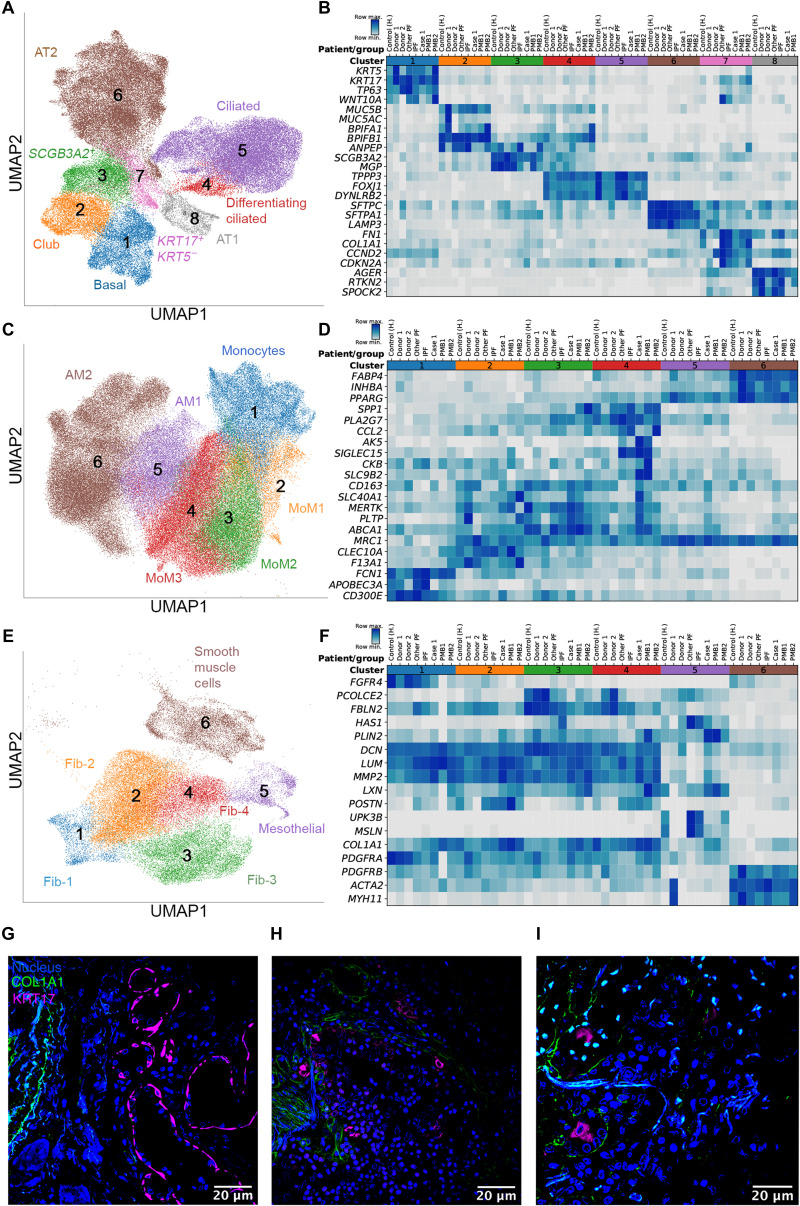
Lung transplantation can potentially be a life-saving treatment for patients with nonresolving COVID-19-associated respiratory failure. Concerns limiting lung transplantation include recurrence of SARS-CoV-2 infection in the allograft, technical challenges imposed by viral-mediated injury to the native lung, and the potential risk for allograft infection by pathogens causing ventilator-associated pneumonia in the native lung. Additionally, the native lung might recover, resulting in long-term outcomes preferable to those of transplant. Here, we report the results of lung transplantation in three patients with nonresolving COVID-19-associated respiratory failure. We performed single-molecule fluorescence in situ hybridization (smFISH) to detect both positive and negative strands of SARS-CoV-2 RNA in explanted lung tissue from the three patients and in additional control lung tissue samples. We conducted extracellular matrix imaging and single-cell RNA sequencing on explanted lung tissue from the three patients who underwent transplantation and on warm postmortem lung biopsies from two patients who had died from COVID-19-associated pneumonia. Lungs from these five patients with prolonged COVID-19 disease were free of SARS-CoV-2 as detected by smFISH, but pathology showed extensive evidence of injury and fibrosis that resembled end-stage pulmonary fibrosis. Using machine learning, we compared single-cell RNA sequencing data from the lungs of patients with late-stage COVID-19 to that from the lungs of patients with pulmonary fibrosis and identified similarities in gene expression across cell lineages. Our findings suggest that some patients with severe COVID-19 develop fibrotic lung disease for which lung transplantation is their only option for survival.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works. Distributed under a Creative Commons Attribution License 4.0 (CC BY).
Figures
Update of
-
Lung transplantation for pulmonary fibrosis secondary to severe COVID-19.medRxiv [Preprint]. 2020 Oct 27:2020.10.26.20218636. doi: 10.1101/2020.10.26.20218636. medRxiv. 2020. Update in: Sci Transl Med. 2020 Dec 16;12(574):eabe4282. doi: 10.1126/scitranslmed.abe4282. PMID: 33140069 Free PMC article. Updated. Preprint.
References
-
- Richardson S., Hirsch J. S., Narasimhan M., Crawford J. M., Ginn T. M., Davidson K. W.; Northwell COVID- Research Consortium, Barnaby D. P., Becker L. B., Chelico J. D., Cohen S. L., Cookingham J., Coppa K., Diefenbach M. A., Dominello A. J., Duer-Hefele J., Falzon L., Gitlin J., Hajizadeh N., Harvin T. G., Hirschwerk D. A., Kim E. J., Kozel Z. M., Marrast L. M., Mogavero J. N., Osorio G. A., Qiu M., Zanos T. P., Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City Area. JAMA 323, 2052–2059 (2020). - PMC - PubMed
-
- McMahon J. H., Udy A., Peleg A. Y., Remdesivir for the treatment of Covid-19 – Preliminary report. N. Engl. J. Med. 383, 992–994 (2020). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
