

Modification of Extracellular Matrix Enhances Oncolytic Adenovirus Immunotherapy in Glioblastoma
- PMID: 33257429
- PMCID: PMC7854507
- DOI: 10.1158/1078-0432.CCR-20-2400
Modification of Extracellular Matrix Enhances Oncolytic Adenovirus Immunotherapy in Glioblastoma
Abstract
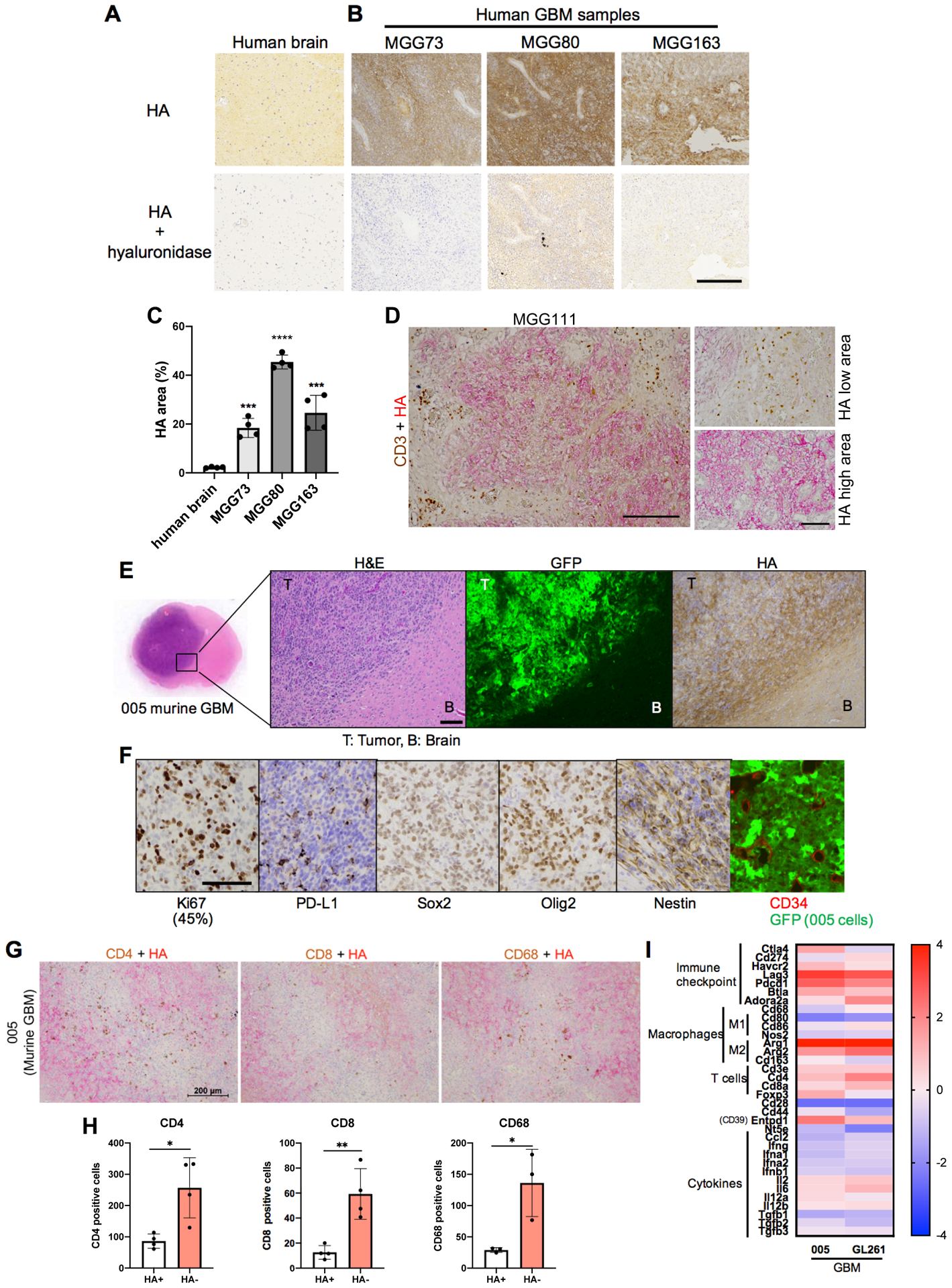
Purpose: Extracellular matrix (ECM) component hyaluronan (HA) facilitates malignant phenotypes of glioblastoma (GBM), however, whether HA impacts response to GBM immunotherapies is not known. Herein, we investigated whether degradation of HA enhances oncolytic virus immunotherapy for GBM.
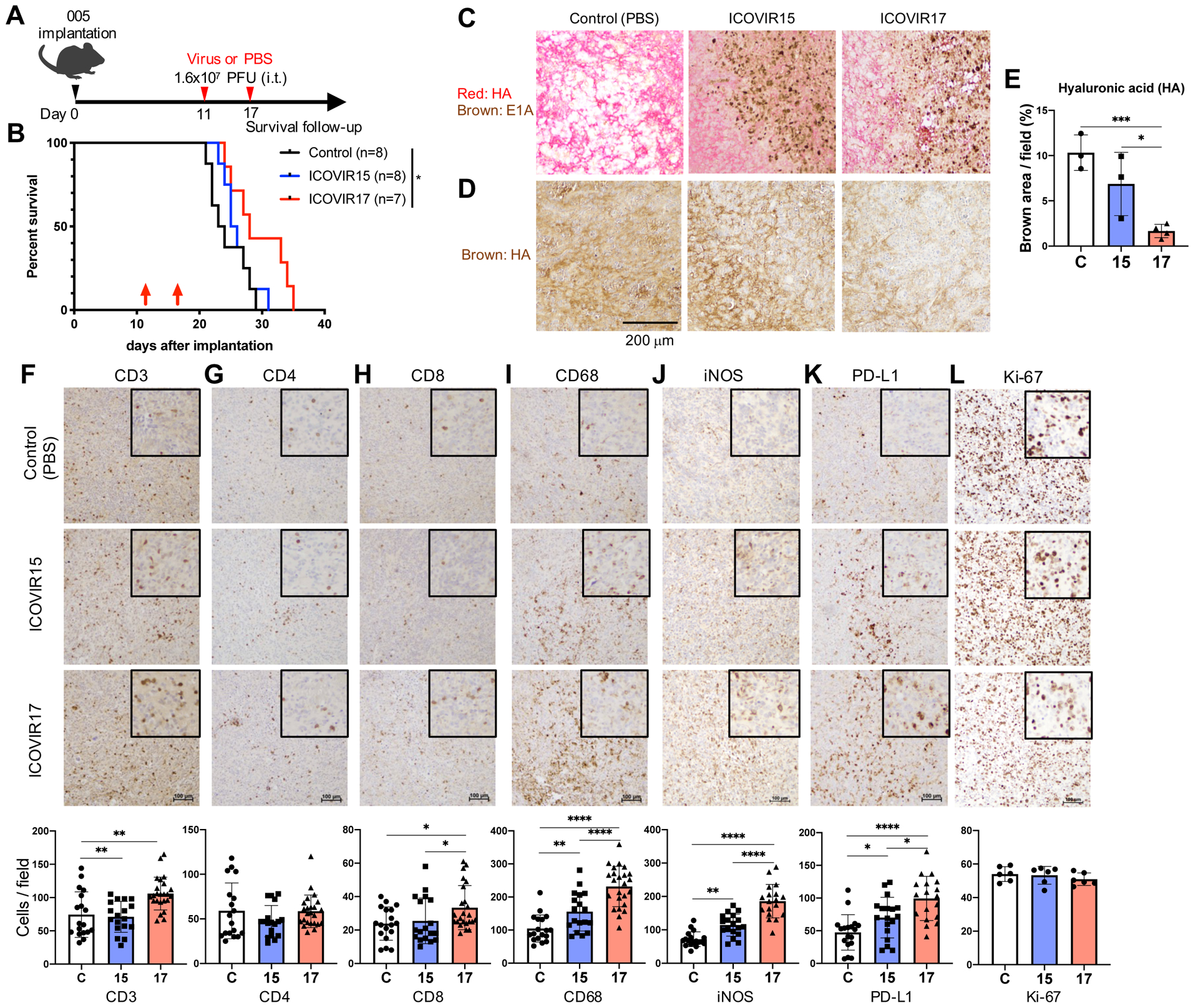
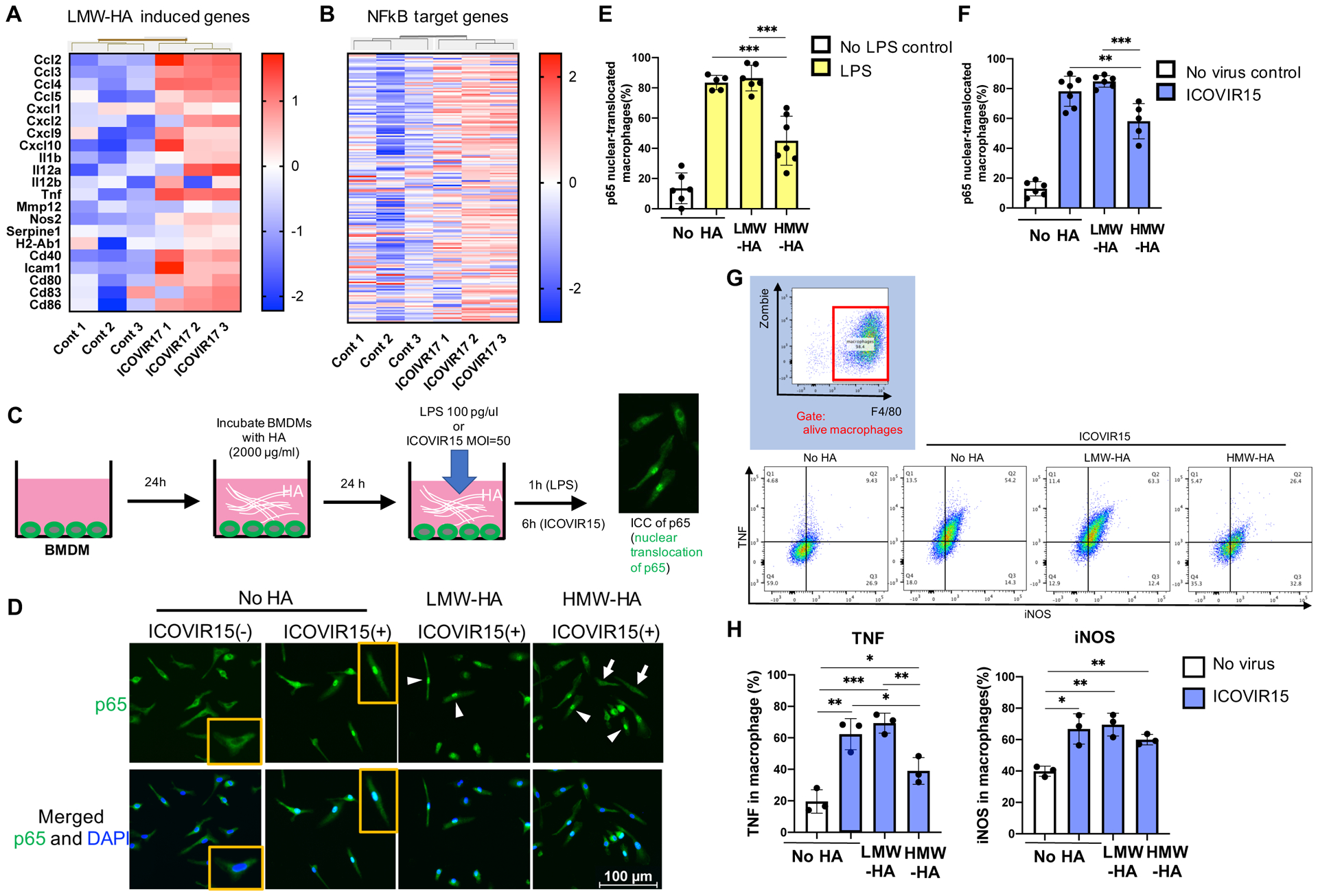
Experimental design: Presence of HA was examined in patient and murine GBM. Hyaluronidase-expressing oncolytic adenovirus, ICOVIR17, and its parental virus, ICOVIR15, without transgene, were tested to determine if they increased animal survival and modulated the immune tumor microenvironment (TME) in orthotopic GBM. HA regulation of NF-κB signaling was examined in virus-infected murine macrophages. We combined ICOVIR17 with PD-1 checkpoint blockade and assessed efficacy and determined mechanistic contributions of tumor-infiltrating myeloid and T cells.
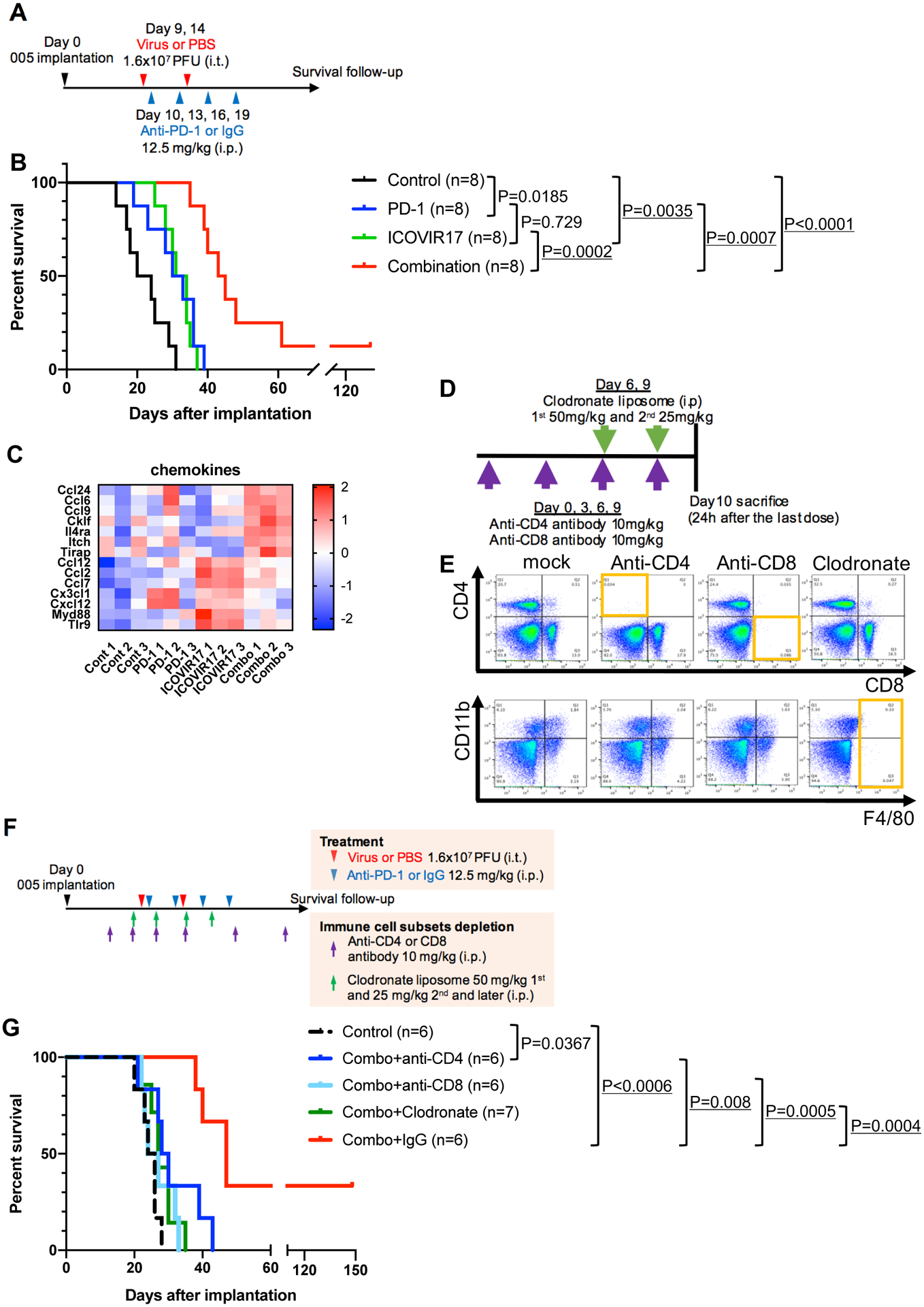
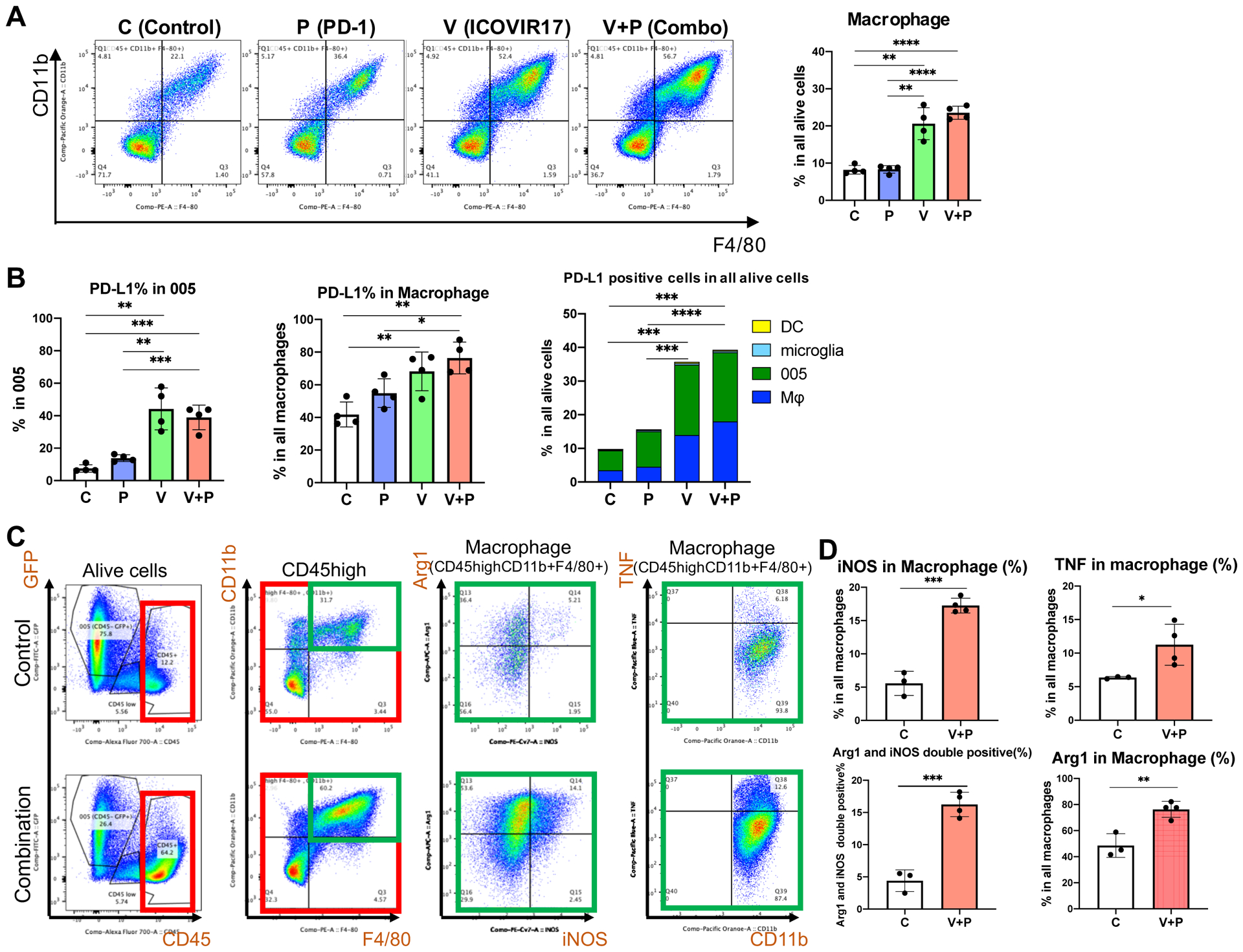
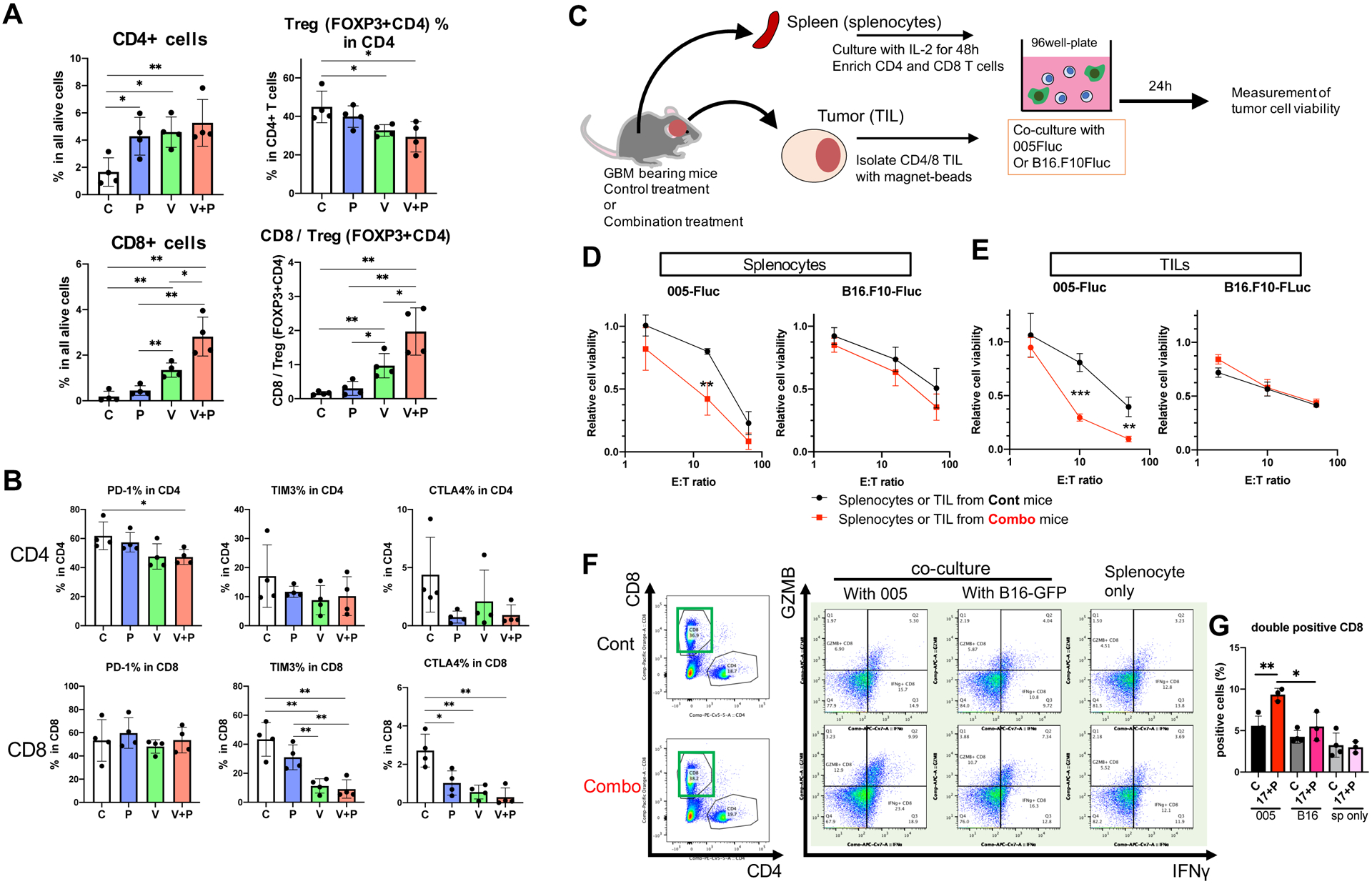
Results: Treatment of murine orthotopic GBM with ICOVIR17 increased tumor-infiltrating CD8+ T cells and macrophages, and upregulated PD-L1 on GBM cells and macrophages, leading to prolonged animal survival, compared with control virus ICOVIR15. High molecular weight HA inhibits adenovirus-induced NF-κB signaling in macrophages in vitro, linking HA degradation to macrophage activation. Combining ICOVIR17 with anti-PD-1 antibody further extended the survival of GBM-bearing mice, achieving long-term remission in some animals. Mechanistically, CD4+ T cells, CD8+ T cells, and macrophages all contributed to the combination therapy that induced tumor-associated proinflammatory macrophages and tumor-specific T-cell cytotoxicity locally and systemically.
Conclusions: Our studies are the first to show that immune modulatory ICOVIR17 has a dual role of mediating degradation of HA within GBM ECM and subsequently modifying the immune landscape of the TME, and offers a mechanistic combination immunotherapy with PD-L1/PD-1 blockade that remodels innate and adaptive immune cells.
©2020 American Association for Cancer Research.
Conflict of interest statement
Conflict of interest disclosore
R. Alemany reports personal fees from VCN Biosciences outside the submitted work, as well as has a patent for hyaluronidase-armed oncolytic adenoviruses issued. S.D. Rabkin reports grants from NIH during the conduct of the study, personal fees from Replimune and from Cellinta outside the submitted work, and coinventor on patents relating to oncolytic herpes simplex viruses, owned and managed by Georgetown University and Massachusetts General Hospital, which have received royalties from Amgen and ActiVec Inc. K. Shah owns equity in and is a member of the Board of Directors, AMASA Therapeutics, Inc., a company developing cell-based therapies for cancer. K. Shah’s interests were reviewed and are managed by Brigham and Women’s Hospital and Partners HealthCare in accordance with their conflict of interest policies. No disclosures were reported by the other authors.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
