

Population Pharmacokinetic and Pharmacokinetic/Pharmacodynamic Analyses of Cefiderocol, a Parenteral Siderophore Cephalosporin, in Patients with Pneumonia, Bloodstream Infection/Sepsis, or Complicated Urinary Tract Infection
- PMID: 33257454
- PMCID: PMC8092503
- DOI: 10.1128/AAC.01437-20
Population Pharmacokinetic and Pharmacokinetic/Pharmacodynamic Analyses of Cefiderocol, a Parenteral Siderophore Cephalosporin, in Patients with Pneumonia, Bloodstream Infection/Sepsis, or Complicated Urinary Tract Infection
Abstract
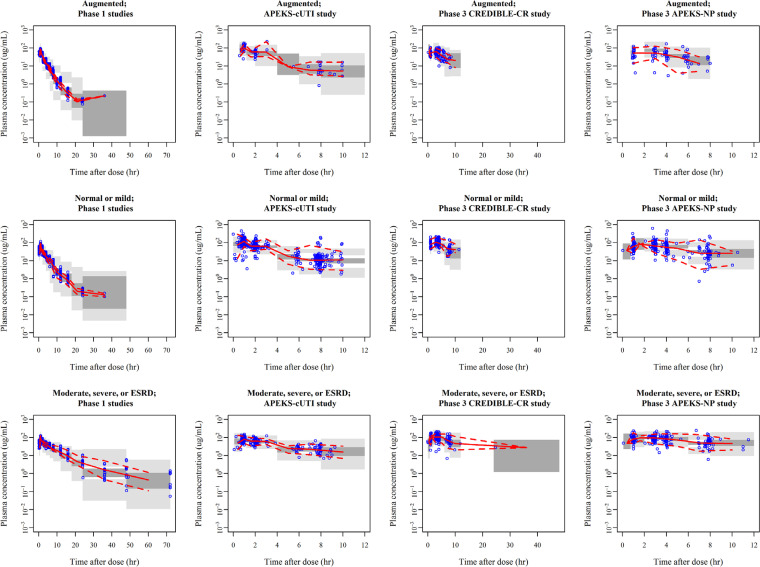
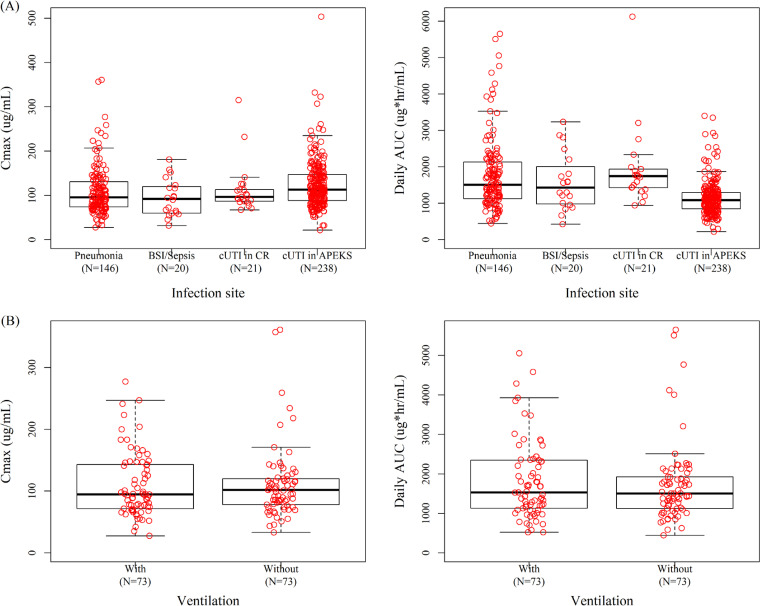
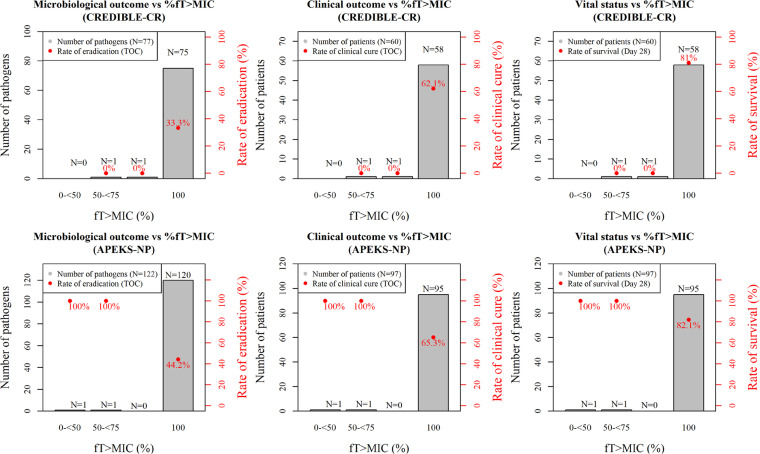
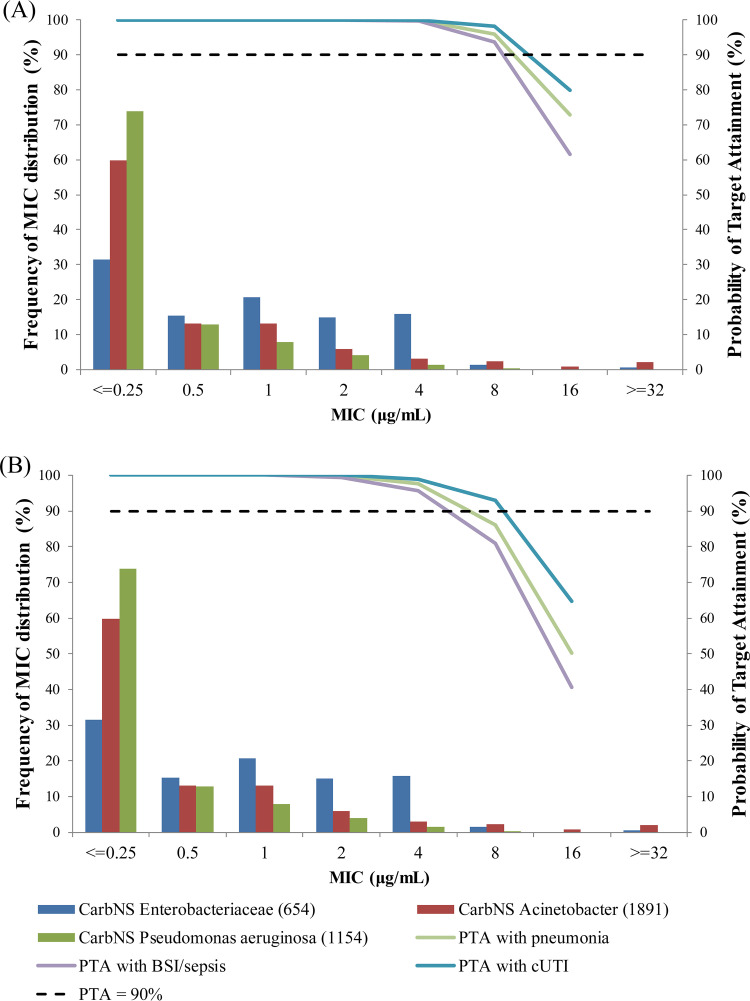
Cefiderocol is a novel siderophore cephalosporin with antibacterial activity against Gram-negative bacteria, including carbapenem-resistant strains. The standard dosing regimen of cefiderocol is 2 g administered every 8 hours over 3 hours infusion in patients with creatinine clearance (CrCL) of 60 to 119 ml/min, and it is adjusted for patients with <60 ml/min or ≥120 ml/min CrCL. A population pharmacokinetic (PK) model was constructed using 3,427 plasma concentrations from 91 uninfected subjects and 425 infected patients with pneumonia, bloodstream infection/sepsis (BSI/sepsis), and complicated urinary tract infection (cUTI). Plasma cefiderocol concentrations were adequately described by the population PK model, and CrCL was the most significant covariate. No other factors, including infection sites and mechanical ventilation, were clinically relevant, although the effect of infection sites was identified as a statistically significant covariate in the population PK analysis. No clear pharmacokinetic/pharmacodynamic relationship was found for any of the microbiological outcome, clinical outcome, or vital status. This is because the estimated percentage of time for which free plasma concentrations exceed the minimum inhibitory concentration (MIC) over dosing interval (%fT>MIC) was 100% in most of the enrolled patients. The probability of target attainment (PTA) for 100% fT>MIC was >90% against MICs of ≤4 μg/ml for all infection sites and renal function groups except for BSI/sepsis patients with normal renal function (85%). These study results support adequate plasma exposure can be achieved at the cefiderocol recommended dosing regimen for the infected patients, including the patients with augmented renal function, ventilation, and/or severe illness.
Keywords: augmented renal function; bloodstream infections; cefiderocol; cephalosporin; complicated urinary tract infection; pharmacodynamics; pneumonia; population pharmacokinetics; ventilation.
Copyright © 2021 Kawaguchi et al.
Figures
References
-
- Kohira N, West J, Ito A, Ito-Horiyama T, Nakamura R, Sato T, Rittenhouse S, Tsuji M, Yamano Y. 2015. In vitro antimicrobial activity of a siderophore cephalosporin, S-649266, against Enterobacteriaceae clinical isolates, including Carbapenem-resistant strains. Antimicrob Agents Chemother 60:729–734. doi:10.1128/AAC.01695-15. - DOI - PMC - PubMed
-
- Ito A, Kohira N, Bouchillon SK, West J, Rittenhouse S, Sader HS, Rhomberg PR, Jones RN, Yoshizawa H, Nakamura R, Tsuji M, Yamano Y. 2016. In vitro antimicrobial activity of S-649266, a catechol-substituted siderophore cephalosporin, when tested against non-fermenting Gram-negative bacteria. J Antimicrob Chemother 71:670–677. doi:10.1093/jac/dkv402. - DOI - PubMed
-
- Ito A, Sato T, Ota M, Takemura M, Nishikawa T, Toba S, Kohira N, Miyagawa S, Ishibashi N, Matsumoto S, Nakamura R, Tsuji M, Yamano Y. 2017. In vitro antibacterial properties of cefiderocol, a novel siderophore cephalosporin, against Gram-negative bacteria. Antimicrob Agents Chemother 62:e01454-17. doi:10.1128/AAC.01454-17. - DOI - PMC - PubMed
-
- Nakamura R, Ito-Horiyama T, Takemura M, Toba S, Matsumoto S, Ikehara T, Tsuji M, Sato T, Yamano Y. 2019. In vivo pharmacodynamic study of cefiderocol, a novel parenteral siderophore cephalosporin, in murine thigh and lung infection models. Antimicrob Agents Chemother 63:e02031-18. doi:10.1128/AAC.02031-18. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
