

A clinically applicable deep-learning model for detecting intracranial aneurysm in computed tomography angiography images
- PMID: 33257700
- PMCID: PMC7705757
- DOI: 10.1038/s41467-020-19527-w
A clinically applicable deep-learning model for detecting intracranial aneurysm in computed tomography angiography images
Abstract
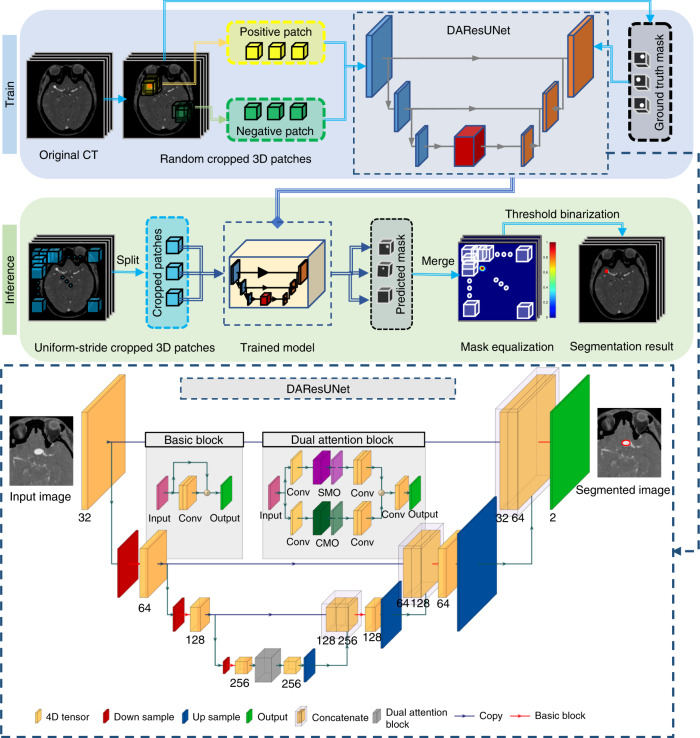
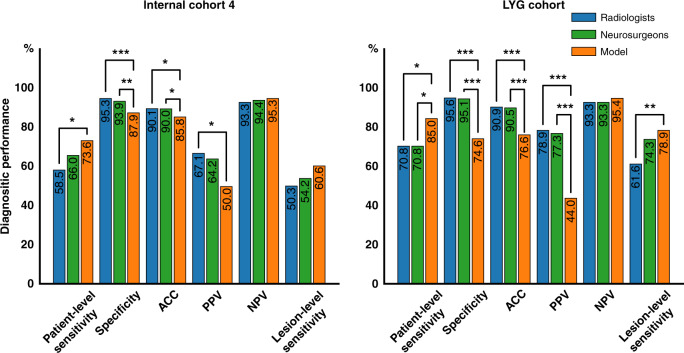
Intracranial aneurysm is a common life-threatening disease. Computed tomography angiography is recommended as the standard diagnosis tool; yet, interpretation can be time-consuming and challenging. We present a specific deep-learning-based model trained on 1,177 digital subtraction angiography verified bone-removal computed tomography angiography cases. The model has good tolerance to image quality and is tested with different manufacturers. Simulated real-world studies are conducted in consecutive internal and external cohorts, in which it achieves an improved patient-level sensitivity and lesion-level sensitivity compared to that of radiologists and expert neurosurgeons. A specific cohort of suspected acute ischemic stroke is employed and it is found that 99.0% predicted-negative cases can be trusted with high confidence, leading to a potential reduction in human workload. A prospective study is warranted to determine whether the algorithm could improve patients' care in comparison to clinicians' assessment.
Conflict of interest statement
Dr. Schoepf receives institutional research support from Bayer, Bracco, Guerbet, HeartFlow, Inc., and Siemens Healthineers and received personal fees for consulting and/or speaking from Bayer, Elucid BioImaging, General Electric, HeartFlow,. Inc., Keya Medical, and Siemens Healthineers. The other authors declare no competing interests.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
