

A systematic review of risk prediction models for perioperative mortality after thoracic surgery
- PMID: 33257987
- PMCID: PMC8906726
- DOI: 10.1093/icvts/ivaa273
A systematic review of risk prediction models for perioperative mortality after thoracic surgery
Abstract
Objectives: Guidelines advocate that patients being considered for thoracic surgery should undergo a comprehensive preoperative risk assessment. Multiple risk prediction models to estimate the risk of mortality after thoracic surgery have been developed, but their quality and performance has not been reviewed in a systematic way. The objective was to systematically review these models and critically appraise their performance.
Methods: The Cochrane Library and the MEDLINE database were searched for articles published between 1990 and 2019. Studies that developed or validated a model predicting perioperative mortality after thoracic surgery were included. Data were extracted based on the checklist for critical appraisal and data extraction for systematic reviews of prediction modelling studies.
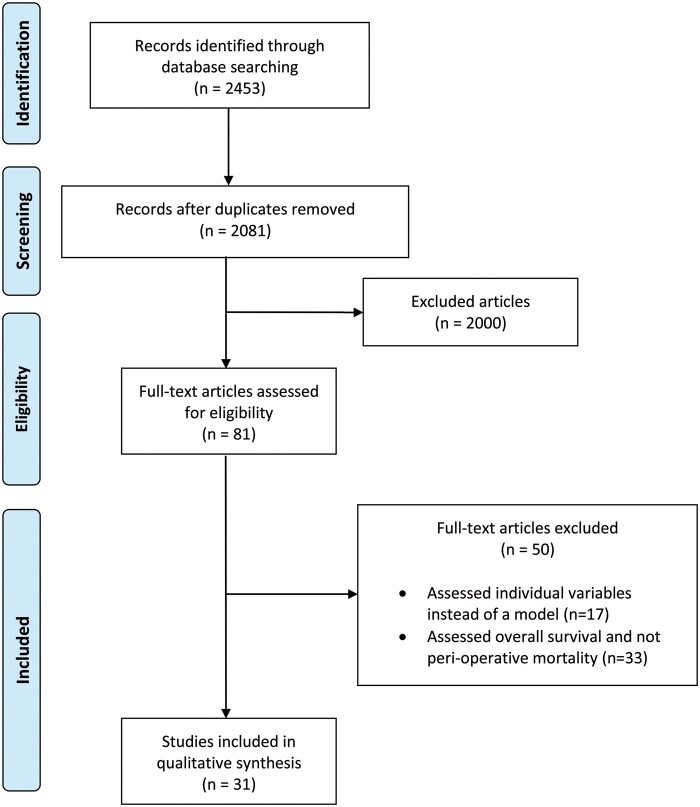
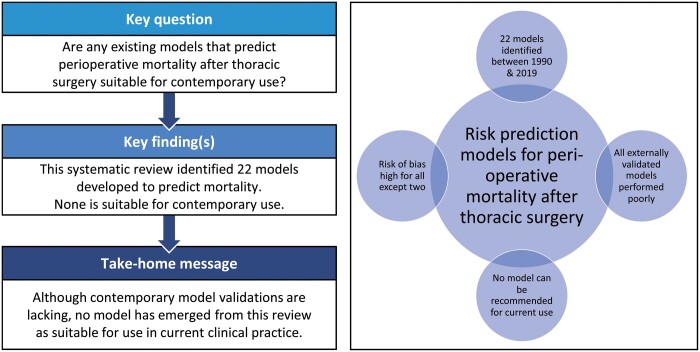
Results: A total of 31 studies describing 22 different risk prediction models were identified. There were 20 models developed specifically for thoracic surgery with two developed in other surgical specialties. A total of 57 different predictors were included across the identified models. Age, sex and pneumonectomy were the most frequently included predictors in 19, 13 and 11 models, respectively. Model performance based on either discrimination or calibration was inadequate for all externally validated models. The most recent data included in validation studies were from 2018. Risk of bias (assessed using Prediction model Risk Of Bias ASsessment Tool) was high for all except two models.
Conclusions: Despite multiple risk prediction models being developed to predict perioperative mortality after thoracic surgery, none could be described as appropriate for contemporary thoracic surgery. Contemporary validation of available models or new model development is required to ensure that appropriate estimates of operative risk are available for contemporary thoracic surgical practice.
Keywords: 90-Day mortality; Perioperative mortality; Risk model; Thoracic surgery.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Similar articles
-
Prediction Models for Prognosis of Cervical Cancer: Systematic Review and Critical Appraisal.Front Public Health. 2021 May 7;9:654454. doi: 10.3389/fpubh.2021.654454. eCollection 2021. Front Public Health. 2021. PMID: 34026714 Free PMC article.
-
Development of a Pediatric Risk Assessment Score to Predict Perioperative Mortality in Children Undergoing Noncardiac Surgery.Anesth Analg. 2017 May;124(5):1514-1519. doi: 10.1213/ANE.0000000000001541. Anesth Analg. 2017. PMID: 27575562
-
Reliability of new scores in predicting perioperative mortality after isolated aortic valve surgery: a comparison with the society of thoracic surgeons score and logistic EuroSCORE.Ann Thorac Surg. 2013 May;95(5):1539-44. doi: 10.1016/j.athoracsur.2013.01.058. Epub 2013 Mar 7. Ann Thorac Surg. 2013. PMID: 23473650
-
Risk Prediction Models for Long-Term Survival after Cardiac Surgery: A Systematic Review.Thorac Cardiovasc Surg. 2024 Jan;72(1):29-39. doi: 10.1055/s-0043-1760747. Epub 2023 Feb 7. Thorac Cardiovasc Surg. 2024. PMID: 36750201
-
Prediction models for the risk of gestational diabetes: a systematic review.Diagn Progn Res. 2017 Feb 8;1:3. doi: 10.1186/s41512-016-0005-7. eCollection 2017. Diagn Progn Res. 2017. PMID: 31093535 Free PMC article. Review.
Cited by
-
Pneumonectomy for primary lung cancer: contemporary outcomes, risk factors and model validation.Interact Cardiovasc Thorac Surg. 2022 Jun 1;34(6):1054-1061. doi: 10.1093/icvts/ivab340. Interact Cardiovasc Thorac Surg. 2022. PMID: 34871415 Free PMC article.
-
Predicting the unpredictable in cardiothoracic surgery.Indian J Thorac Cardiovasc Surg. 2023 Mar;39(2):109-111. doi: 10.1007/s12055-023-01478-8. Epub 2023 Jan 26. Indian J Thorac Cardiovasc Surg. 2023. PMID: 36785611 Free PMC article. No abstract available.
-
Lung Metastasectomy: Where Do We Stand? Results from an Italian Multicentric Prospective Database.J Clin Med. 2024 May 25;13(11):3106. doi: 10.3390/jcm13113106. J Clin Med. 2024. PMID: 38892816 Free PMC article.
-
Does the Performance of a Six-Minute Walking Test Predict Cardiopulmonary Complications After Uniportal Video-Assisted Thoracic Surgery Anatomic Lung Resection?Cancers (Basel). 2024 Dec 26;17(1):32. doi: 10.3390/cancers17010032. Cancers (Basel). 2024. PMID: 39796663 Free PMC article.
References
-
- Lim E, Baldwin D, Beckles M, Duffy J, Entwisle J, Faivre-Finn C. et al. Guidelines on the radical management of patients with lung cancer. Thorax 2010;65:iii1–27. - PubMed
-
- Detterbeck FC, Lewis SZ, Diekemper R, Addrizzo-Harris D, Alberts WM.. Executive Summary: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:7S–37S. - PubMed
-
- Brunelli A, Charloux A, Bolliger CT, Rocco G, Sculier JP, Varela G. et al. ERS/ESTS clinical guidelines on fitness for radical therapy in lung cancer patients (surgery and chemo-radiotherapy). Eur Respir J 2009;34:17–41. - PubMed
-
- National Institute for Health and Care Excellence. Lung Cancer: Diagnosis and Management (NICE Guideline 122). Available at www.nice.org.uk/guidance/ng122. 2019. - PubMed
-
- Shahian DM, Edwards FH.. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: introduction. Ann Thorac Surg 2009;88(Suppl 1):S1. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
