

Congestive nephropathy: a neglected entity? Proposal for diagnostic criteria and future perspectives
- PMID: 33258308
- PMCID: PMC7835563
- DOI: 10.1002/ehf2.13118
Congestive nephropathy: a neglected entity? Proposal for diagnostic criteria and future perspectives
Abstract
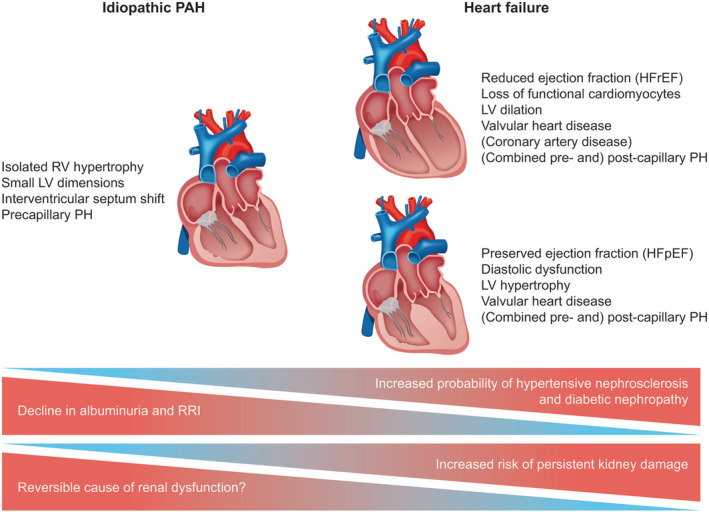
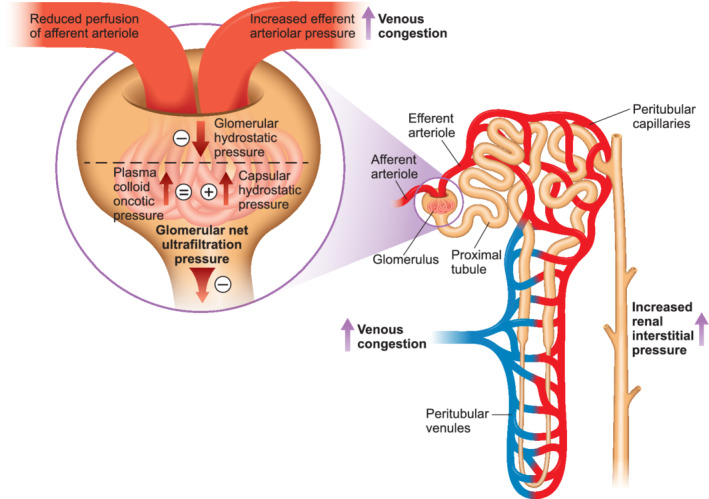
Venous congestion has emerged as an important cause of renal dysfunction in patients with cardiorenal syndrome. However, only limited progress has been made in differentiating this haemodynamic phenotype of renal dysfunction, because of a significant overlap with pre-existing renal impairment due to long-term hypertension, diabetes, and renovascular disease. We propose congestive nephropathy (CN) as this neglected clinical entity. CN is a potentially reversible subtype of renal dysfunction associated with declining renal venous outflow and progressively increasing renal interstitial pressure. Venous congestion may lead to a vicious cycle of hormonal activation, increased intra-abdominal pressure, excessive renal tubular sodium reabsorption, and volume overload, leading to further right ventricular (RV) stress. Ultimately, renal replacement therapy may be required to relieve diuretic-resistant congestion. Effective decongestion could preserve or improve renal function. Congestive acute kidney injury may not be associated with cellular damage, and complete renal function restoration may be a confirmatory diagnostic criterion. In contrast, a persistently low renal perfusion pressure might induce renal dysfunction and histopathological lesions with time. Thus, urinary markers may differ. CN is mostly seen in biventricular heart failure but may also occur secondary to pulmonary arterial hypertension and elevated intra-abdominal pressure. An increase in central venous pressure to >6 mmHg is associated with a steep decrease in glomerular filtration rate. However, the central venous pressure range that can provide an optimal balance of RV and renal function remains to be determined. We propose criteria to identify cardiorenal syndrome subgroups likely to benefit from decongestive or pulmonary hypertension-specific therapies and suggest areas for future research.
Keywords: Cardiorenal syndromes; Heart failure; Intra-abdominal hypertension; Pulmonary hypertension; Venous congestion.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
Dr. Gall discloses personal fees and non‐financial support from Actelion, AstraZeneca, Bayer, BMS, GlaxoSmithKline, Janssen Cilag, Lilly, MSD, Novartis, Pfizer, and United Therapeutics/OMT outside the submitted work. Dr. Seeger discloses personal fees for consulting from Bayer Pharma AG, from Liquidia Technologies, Inc, and from United Therapeutics Corporation outside the submitted work. Dr. Ghofrani discloses grants from German Research Foundation (DFG) during the conduct of the study and personal fees from Actelion, Bayer, GSK, Novartis, Pfizer, Bellerophon Pulse Technologies, and MSD Merck Sharpe & Dohme outside the submitted work. None of the other authors declare any competing interests.
Figures
References
-
- Damman K, van Deursen VM, Navis G, Voors AA, van Veldhuisen DJ, Hillege HL. Increased central venous pressure is associated with impaired renal function and mortality in a broad spectrum of patients with cardiovascular disease. J Am Coll Cardiol 2009; 53: 582–588. - PubMed
-
- Husain‐Syed F, McCullough PA, Birk HW, Renker M, Brocca A, Seeger W, Ronco C. Cardio‐pulmonary‐renal interactions: a multidisciplinary approach. J Am Coll Cardiol 2015; 65: 2433–2448. - PubMed
-
- Verbrugge FH, Dupont M, Steels P, Grieten L, Malbrain M, Tang WH, Mullens W. Abdominal contributions to cardiorenal dysfunction in congestive heart failure. J Am Coll Cardiol 2013; 62: 485–495. - PubMed
-
- Costanzo MR, Ronco C, Abraham WT, Agostoni P, Barasch J, Fonarow GC, Gottlieb SS, Jaski BE, Kazory A, Levin AP, Levin HR, Marenzi G, Mullens W, Negoianu D, Redfield MM, Tang WHW, Testani JM, Voors AA. Extracorporeal ultrafiltration for fluid overload in heart failure: current status and prospects for further research. J Am Coll Cardiol 2017; 69: 2428–2445. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical