

High seroprevalence but short-lived immune response to SARS-CoV-2 infection in Paris
- PMID: 33259646
- PMCID: PMC7753614
- DOI: 10.1002/eji.202049058
High seroprevalence but short-lived immune response to SARS-CoV-2 infection in Paris
Abstract
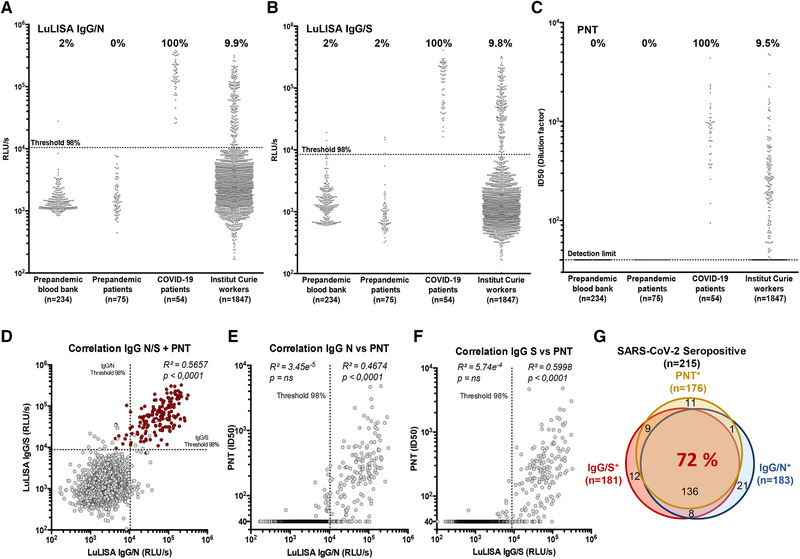
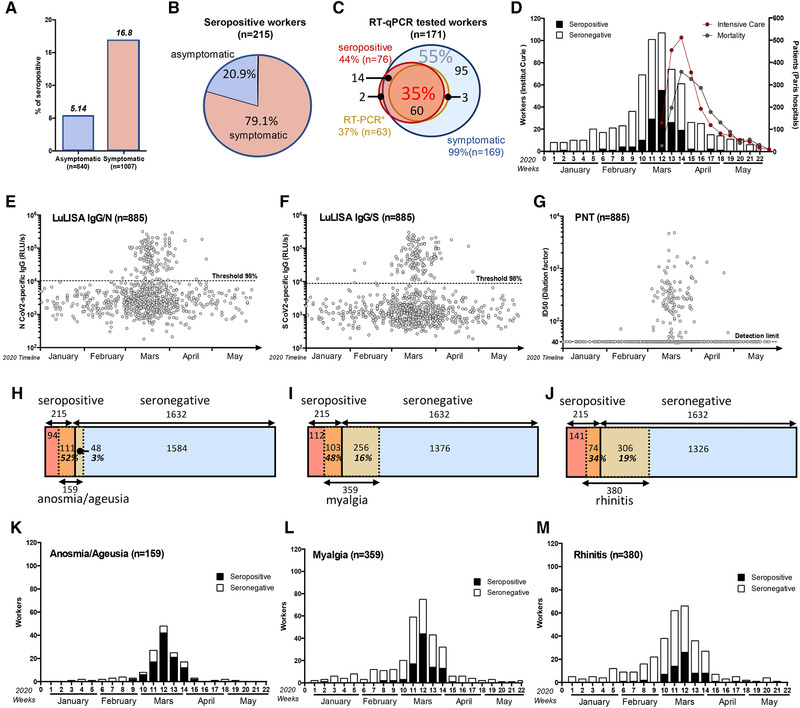
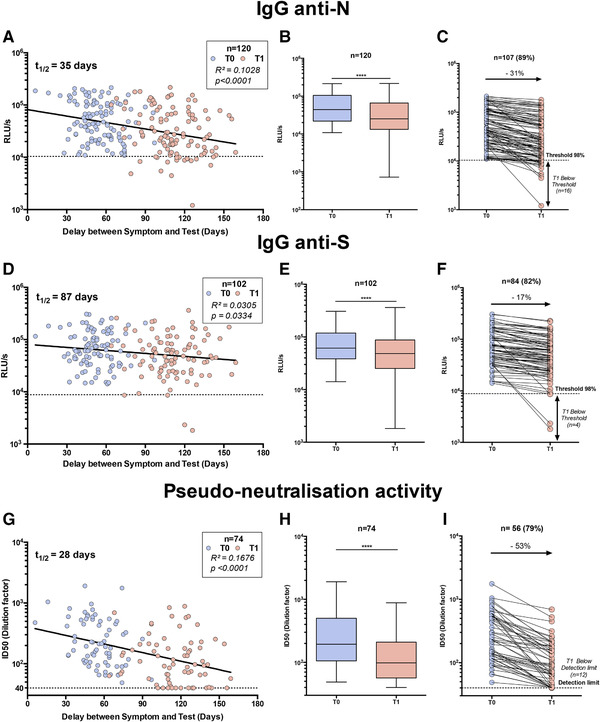
Although the COVID-19 pandemic peaked in March/April 2020 in France, the prevalence of infection is barely known. Using high-throughput methods, we assessed herein the serological response against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) of 1847 participants working in three sites of an institution in Paris conurbation. In May-July 2020, 11% (95% confidence interval [CI]: 9.7-12.6) of serums were positive for IgG against the SARS-CoV-2 N and S proteins, and 9.5% (95% CI: 8.2-11.0) were neutralizer in pseudo-typed virus assays. The prevalence of seroconversion was 11.6% (95% CI: 10.2-13.2) when considering positivity in at least one assay. In 5% of RT-qPCR positive individuals, no systemic IgGs were detected. Among immune individuals, 21% had been asymptomatic. Anosmia (loss of smell) and ageusia (loss of taste) occurred in 52% of the IgG-positive individuals and in 3% of the negative ones. In contrast, 30% of the anosmia-ageusia cases were seronegative, suggesting that the true prevalence of infection may have reached 16.6%. In sera obtained 4-8 weeks after the first sampling, anti-N and anti-S IgG titers and neutralization activity in pseudo-virus assay declined by 31%, 17%, and 53%, resulting thus in half-life of 35, 87, and 28 days, respectively. The population studied is representative of active workers in Paris. The short lifespan of the serological systemic responses suggests an underestimation of the true prevalence of infection.
Keywords: COVID-19; ELISA; LuLISA; SARS-CoV-2; bioluminescence.
© 2020 Wiley-VCH GmbH.
Conflict of interest statement
YJ, SG, and TR have patented the proluciferins (hikarazines) synthesis and uses (EP 3395803/WO 2018197727, 2018) and applied for a patent, which includes claims describing the LuLISA. FA and PC have applied for a patent claiming the PNT. The rest of the authors declare no commercial or financial conflict of interest.
Figures
References
-
- Wolfel, R. , Corman, V. M. , Guggemos, W. , Seilmaier, M. , Zange, S. , Muller, M. A. , Niemeyer, D. et al., Virological assessment of hospitalized patients with COVID‐2019. Nature 2020. 581: 465–469. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
