

Maternal Morbidity and Mortality: Are We Getting to the "Heart" of the Matter?
- PMID: 33259740
- PMCID: PMC8020498
- DOI: 10.1089/jwh.2020.8852
Maternal Morbidity and Mortality: Are We Getting to the "Heart" of the Matter?
Abstract
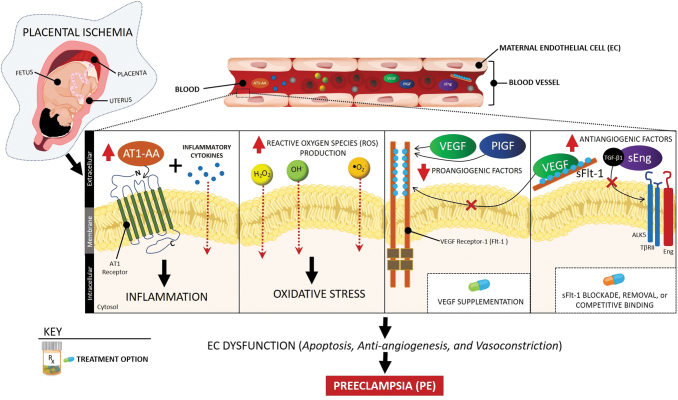
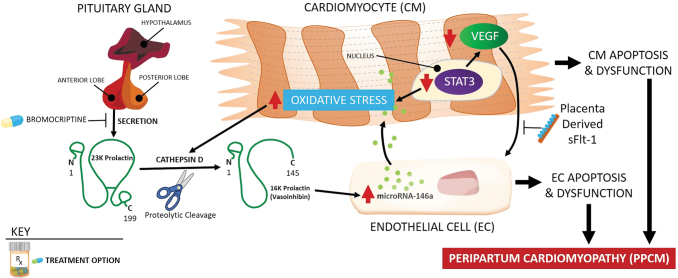
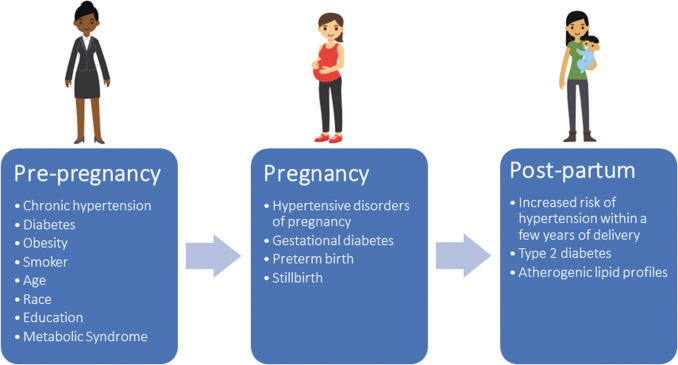
Cardiovascular disease (CVD), including hypertensive disorders of pregnancy (HDP) and peripartum cardiomyopathy, is a leading cause of pregnancy-related death in the United States. Women who are African American or American Indian/Alaskan Native, have HDP, are medically underserved, are older, or are obese have a major risk for the onset and/or progression of CVD during and after pregnancy. Paradoxically, women with no preexisting chronic conditions or risk factors also experience significant pregnancy-related cardiovascular (CV) complications. The question remains whether substantial physiologic stress on the CV system during pregnancy reflected in hemodynamic, hematological, and metabolic changes uncovers subclinical prepregnancy CVD in these otherwise healthy women. Equally important and similarly understudied is the concept that women's long-term CV health could be detrimentally affected by adverse pregnancy outcomes, such as preeclampsia, gestational hypertension, and diabetes, and preterm birth. Thus, a critical life span perspective in the assessment of women's CV risk factors is needed to help women and health care providers recognize and appreciate not only optimal CV health but also risk factors present before, during, and after pregnancy. In this review article, we highlight new advancements in understanding adverse, pregnancy-related CV conditions and will discuss promising strategies or interventions for their prevention, diagnosis, and treatment.
Keywords: adverse pregnancy outcomes; hypertensive disorders of pregnancy; long-term pregnancy-related cardiovascular disease; maternal mortality and morbidity; peripartum cardiomyopathy.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Mehta LS, Warnes CA, Bradley E, et al. . Cardiovascular considerations in caring for pregnant patients: A scientific statement from the American Heart Association. Circulation 2020;141:e884–e903 - PubMed
-
- ACOG Practice Bulletin No. 222: Gestational hypertension and preeclampsia. Obstet Gynecol 2020;135:e237–e260 - PubMed
-
- Berg CJ, Callaghan WM, Henderson Z, Syverson C. Pregnancy-related mortality in the United States, 1998 to 2005. Obstet Gynecol 2011;117:1230 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical