

Spinal Deformities after Childhood Tumors
- PMID: 33260742
- PMCID: PMC7759932
- DOI: 10.3390/cancers12123555
Spinal Deformities after Childhood Tumors
Abstract
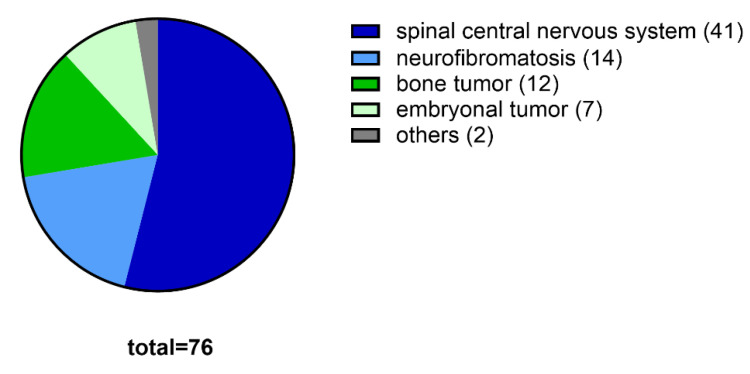
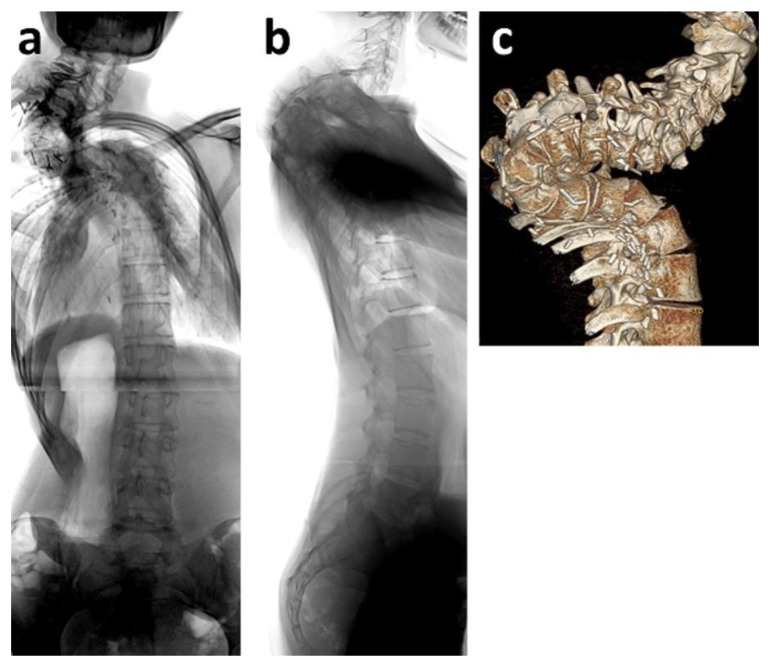
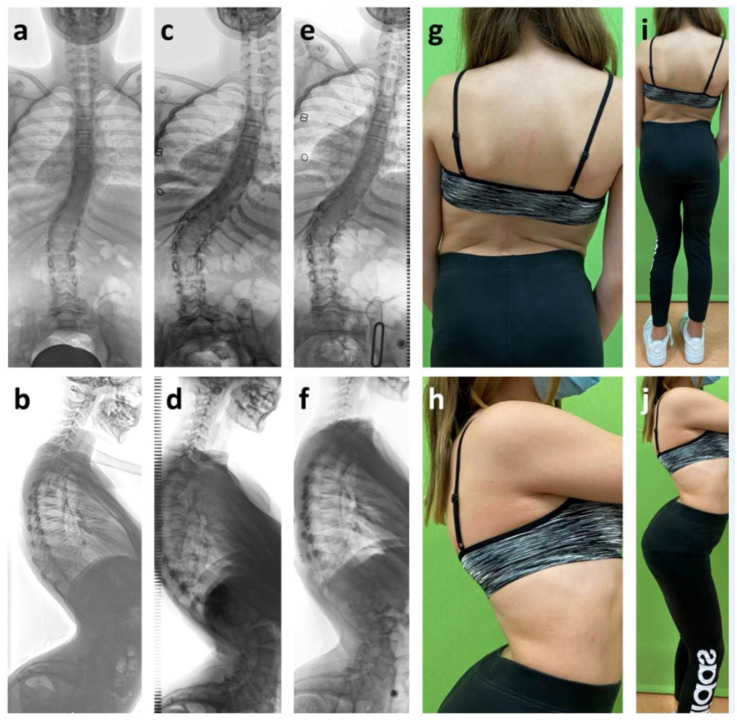
Childhood tumors of the central nervous system (CNS) and other entities affecting the spine are rare. Treatment options vary from surgical biopsy to partial, subtotal, and total resection, to radiation, to chemotherapy. The aim of this study is to investigate spinal deformity and subsequent surgical interventions in this patient cohort. A retrospective review at our institution identified children with CNS tumors, spinal tumors, and juxta-spinal tumors, as well as spinal deformities. Tumor entity, treatment, mobilization, and radiographic images were analyzed relative to the spinal deformity, using curve angles in two planes. Conservative or surgical interventions such as orthotic braces, growth-friendly spinal implants, and spinal fusions were evaluated and analyzed with respect to treatment results. Tumor entities in the 76 patients of this study included CNS tumors (n = 41), neurofibromatosis with spinal or paraspinal tumors (n = 14), bone tumors (n = 12), embryonal tumors (n = 7), and others (n = 2). The initial treatment consisted of surgical biopsy (n = 5), partial, subtotal, or total surgical resection (n = 59), or none (n = 12), followed by chemotherapy, radiotherapy, or both (n = 40). Out of 65 evaluated patients, 25 revealed a moderate or severe scoliotic deformity of 71° (range 21-116°), pathological thoracic kyphosis of 66° (range 50-130°), and lordosis of 61° (range 41-97°). Surgical treatment was performed on 21 patients with implantation of growth-friendly spinal implants (n = 9) as well as twelve dorsal spinal fusions (two with prior halo distraction). Surgical interventions significantly improved spinal deformities without additional neurological impairment. With the increasing number of children surviving rare tumors, attention should be focused on long-term problems such as spinal deformities and consequent disabilities. A significant number of children with CNS tumors, spinal tumors or juxta-spinal tumors required surgical intervention. Early information about spinal deformities and a close follow-up are mandatory for this patient group.
Keywords: central nervous system; children; intramedullary spinal cord tumor; spinal deformity; treatment; tumor.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Yao K.C., McGirt M.J., Chaichana K.L., Constantini S., Jallo G.I. Risk factors for progressive spinal deformity following resection of intramedullary spinal cord tumors in children: An analysis of 161 consecutive cases. J. Neurosurg. Pediatr. 2007;107:463–468. doi: 10.3171/PED-07/12/463. - DOI - PubMed
-
- Papagelopoulos P.J., Peterson H.A., Ebersold M.J., Emmanuel R.P., Choudhury S.N., Quast L.M. Spinal Column Deformity and Instability after Lumbar or Thoracolumbar Laminectomy for Intraspinal Tumors in Children and Young Adults. Spine. 1997;22:442–451. doi: 10.1097/00007632-199702150-00019. - DOI - PubMed
-
- McGirt M.J., Chaichana K.L., Atiba A., Bydon A., Witham T.F., Yao K.C., Jallo G.I. Incidence of spinal deformity after resection of intramedullary spinal cord tumors in children who underwent laminectomy compared with laminoplasty. J. Neurosurg. Pediatr. 2008;1:57–62. doi: 10.3171/PED-08/01/057. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
