

Nanoparticles and Nanostructured Surface Fabrication for Innovative Cranial and Maxillofacial Surgery
- PMID: 33260938
- PMCID: PMC7731022
- DOI: 10.3390/ma13235391
Nanoparticles and Nanostructured Surface Fabrication for Innovative Cranial and Maxillofacial Surgery
Abstract
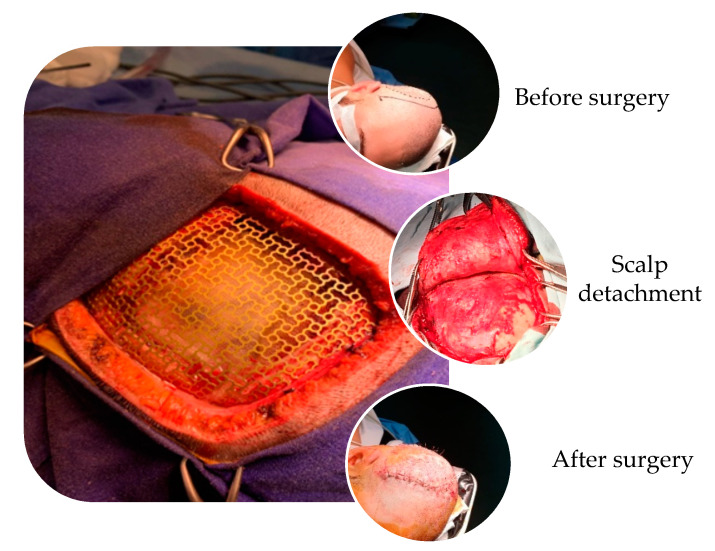
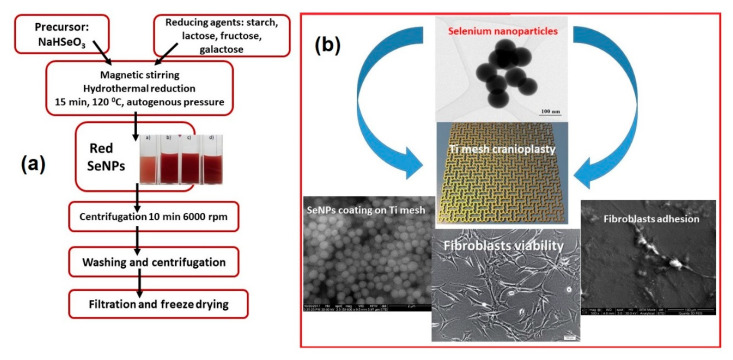
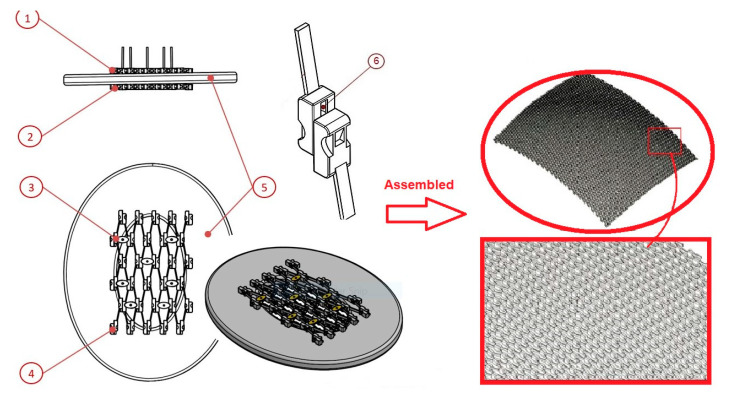
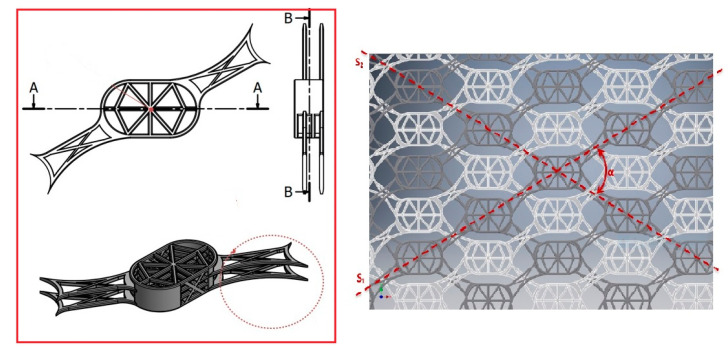
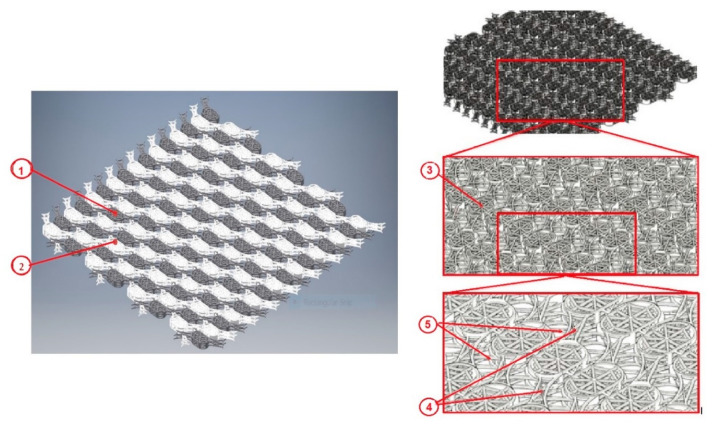
A novel strategy to improve the success of soft and hard tissue integration of titanium implants is the use of nanoparticles coatings made from basically any type of biocompatible substance, which can advantageously enhance the properties of the material, as compared to its similar bulk material. So, most of the physical methods approaches involve the compaction of nanoparticles versus micron-level particles to yield surfaces with nanoscale grain boundaries, simultaneously preserving the chemistry of the surface among different topographies. At the same time, nanoparticles have been known as one of the most effective antibacterial agents and can be used as effective growth inhibitors of various microorganisms as an alternative to antibiotics. In this paper, based on literature research, we present a comprehensive review of the mechanical, physical, and chemical methods for creating nano-structured titanium surfaces along with the main nanoparticles used for the surface modification of titanium implants, the fabrication methods, their main features, and the purpose of use. We also present two patented solutions which involve nanoparticles to be used in cranioplasty, i.e., a cranial endoprosthesis with a sliding system to repair the traumatic defects of the skull, and a cranial implant based on titanium mesh with osteointegrating structures and functional nanoparticles. The main outcomes of the patented solutions are: (a) a novel geometry of the implant that allow both flexible adaptation of the implant to the specific anatomy of the patient and the promotion of regeneration of the bone tissue; (b) porous structure and favorable geometry for the absorption of impregnated active substances and cells proliferation; (c) the new implant model fit 100% on the structure of the cranial defect without inducing mechanical stress; (d) allows all kinds of radiological examinations and rapid osteointegration, along with the patient recover in a shorter time.
Keywords: endoprosthesis; patented solutions; titanium cranioplasty.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Sanan A., Haines S.J. Repairing holes in the head: A history of cranioplasty. Neurosurgery. 1997;40:588–603. - PubMed
-
- Prolo D.J., Oklund S.A. Composite autogeneic human cranioplasty: Frozen skull supplemented with fresh iliac corticocancellous bone. Neurosurgery. 1984;15:846–851. - PubMed
-
- Kwarcinski J., Boughton P., Ruys A., Doolan A., Van Gelder J. Cranioplasty and Craniofacial Reconstruction: A Review of Implant Material, Manufacturing Method and Infection Risk. Appl. Sci. 2017;7:276. doi: 10.3390/app7030276. - DOI
Publication types
LinkOut - more resources
Full Text Sources
