

Hemostatic Balance in Severe Trauma
- PMID: 33262965
- PMCID: PMC7687220
- DOI: 10.3389/fped.2020.600501
Hemostatic Balance in Severe Trauma
Abstract
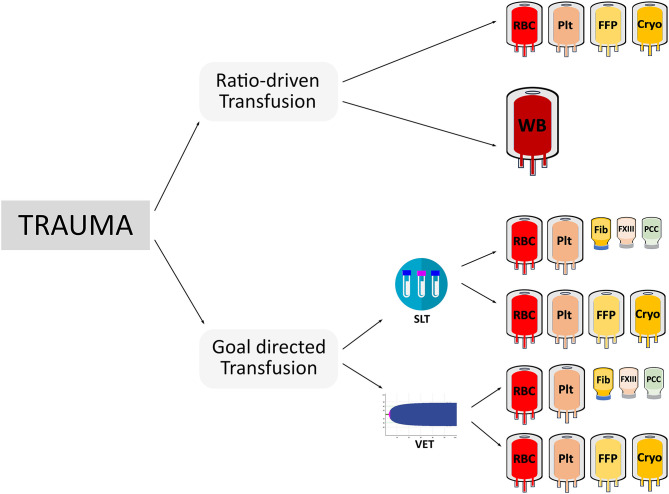
Acute coagulopathy is prevalent in adult and pediatric trauma patients and is associated with increased morbidity and mortality. While reasonable hypotheses have been created to explain the underlying perturbations of adult trauma coagulopathy (i.e., tissue factor-related increase in thrombin generation, protein C activation, hypoperfusion, and hyperfibrinolysis), only a small number of studies have been performed to prove whether these mechanisms can likewise be detected in pediatric trauma patients. In addition, severe hypofibrinogenemia (<100 mg/dL) is a frequent finding in pediatric trauma patients (>20%). Although the probability of life-threatening coagulopathy is low with minor to moderate injury, it is present in almost all patients with an injury severity score >25, hypotension, hypothermia, and acidosis. As these multifactorial changes in hemostasis cannot be adequately and rapidly measured using standard laboratory testing, the use of viscoelastic measurements has been established in adult trauma management, but prospective studies in children are urgently needed. Apart from diagnostic challenges, several studies have focused on the impact of blood product ratios on the treatment of massively bleeding pediatric trauma patients. The majority of these studies were unable to show improved survival by using higher plasma to red blood cell ratios or higher platelet to red blood cells ratios, but there are no published randomized trials to definitively answer this question. A goal-directed transfusion protocol using viscoelastic tests together with early substitution with an antifibrinolytic and fibrinogen replacement is a promising alternative to traditional ratio-based interventions. Another crucial factor in treating trauma-induced coagulopathy is the early detection of hypofibrinogenemia, a common condition in massively transfused patients. Early treatment of hypofibrinogenemia is associated with improved morbidity and mortality in adults, but needs to be further studied in future pediatric trials. Pediatric trauma patients are not only threatened by coagulopathy-related bleeding but are also at higher risk for venous thromboembolism. Pediatric trauma patients with brain injury, central venous catheters, immobilization, or surgical procedures are at highest risk for developing a deep venous thrombosis. There are no specific pediatric guidelines established to prevent venous thromboembolism in children suffering from traumatic injury.
Keywords: coagulation factor concentrates; massive bleeding; pediatrics; thrombosis; transfusion; trauma; viscoelastic testing.
Copyright © 2020 Haas and Cushing.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials