

Gender does not impact the short- or long-term outcomes of home-based pulmonary rehabilitation in patients with COPD
- PMID: 33263025
- PMCID: PMC7682653
- DOI: 10.1183/23120541.00032-2020
Gender does not impact the short- or long-term outcomes of home-based pulmonary rehabilitation in patients with COPD
Abstract
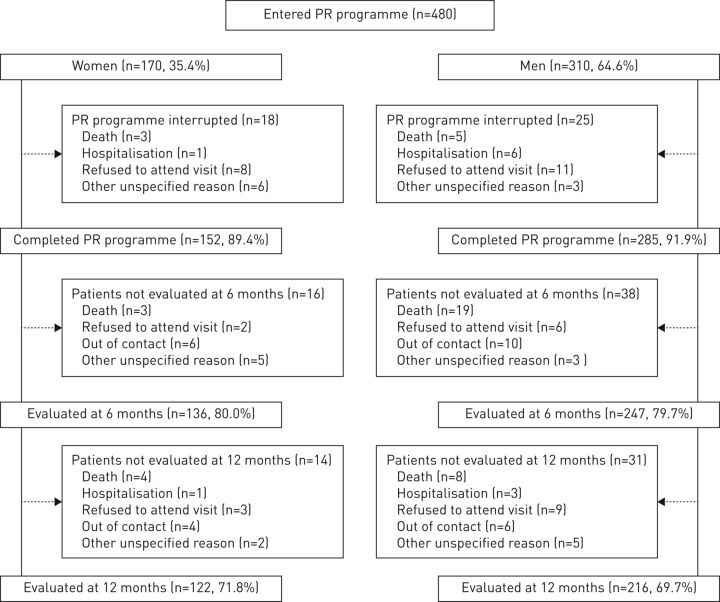
Pulmonary rehabilitation, whether performed at home or in a specialised centre, is effective in the management of COPD. As gender-related differences in COPD were previously reported, we aimed to evaluate the impact of gender on pulmonary rehabilitation outcomes in the short, medium and long term. In this retrospective observational study of 170 women and 310 men with COPD, we compared the outcomes of an 8-week home-based pulmonary rehabilitation programme including an individualised plan of retraining exercises, physical activities, therapeutic education, and psychosocial and self-management support. Exercise tolerance, anxiety, depression, and quality of life (QOL) were assessed using the 6-min stepper test (6MST), Hospital Anxiety and Depression Scale (HADS) and Visual Simplified Respiratory Questionnaire (VSRQ), respectively. Assessments were carried out before, immediately after the pulmonary rehabilitation programme (T2) and at 8 (T8) and 14 months (T14). At baseline, women were younger (mean 62.1 versus 65.3 years), more often nonsmokers (24.7% versus 7.7%) and had a higher body mass index (28 versus 26.4 kg·m-2). They more often lived alone (50.6% versus 24.5%) and experienced social deprivation (66.7% versus 56.4%). They had significantly lower exercise tolerance (-34 strokes, 6MST) and higher anxiety and depression (+3.2 HADS total score), but there were no between gender differences in QOL (VSRQ). Both groups showed similar improvements in all outcome measures at T2, T8 and T14 with a tendency for men to lose QOL profits over time. Despite some differences in baseline characteristics, women and men with COPD had similar short-, medium- and long-term benefits of a home-based pulmonary rehabilitation programme.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: J-M. Grosbois reports FormAction Santé (J-M. Grosbois) received financial support from Adair, Aeris Santé, Bastide, France Oxygène, Homeperf, LVL Medical, Medopale, NorOx, Santélys, Santeo, SOS Oxygène, Sysmed, VitalAire and the ARS Hauts de France for the home-based pulmonary rehabilitation programme; personal fees and nonfinancial support from AstraZeneca and Boehringer Ingelheim, personal fees from Chiesi, nonfinancial support from GlaxoSmithKline and Novartis, and personal fees from Vitalaire and Roche, during the conduct of the study. Conflict of interest: S. Gephine has nothing to disclose. Conflict of interest: A.S. Diot has nothing to disclose. Conflict of interest: M. Kyheng has nothing to disclose. Conflict of interest: F. Machuron has nothing to disclose. Conflict of interest: G. Terce has nothing to disclose. Conflict of interest: B. Wallaert reports personal fees and nonfinancial support from Roche and Boehringer Ingelheim, and nonfinancial support from Vitalaire, outside the submitted work. Conflict of interest: C. Chenivesse reports grants from AstraZeneca and Santélys, personal fees from ALK-Abello, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Roche, Sanofi and TEVA, and nonfinancial support from ALK-Abello, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, MEDA Pharma, Medexact, Novartis, Pierre Fabre and Pfizer, outside the submitted work. Conflict of interest: O. Le Rouzic reports personal fees and nonfinancial support from AstraZeneca, Boehringer Ingelheim, Chiesi, Lilly and Novartis, and nonfinancial support from GlaxoSmithKline, MundiPharma, Pfizer, Teva, Santelys Association, Vertex and Vitalaire, outside the submitted work.
Figures


References
-
- Ni H, Xu J. COPD-related mortality by sex and race among adults aged 25 and over: United States, 2000–2014. NCHS Data Brief 2016; 256: 1–8. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials