

Prediction of lung function and lung density of young adults who had bronchopulmonary dysplasia
- PMID: 33263029
- PMCID: PMC7682661
- DOI: 10.1183/23120541.00157-2020
Prediction of lung function and lung density of young adults who had bronchopulmonary dysplasia
Abstract
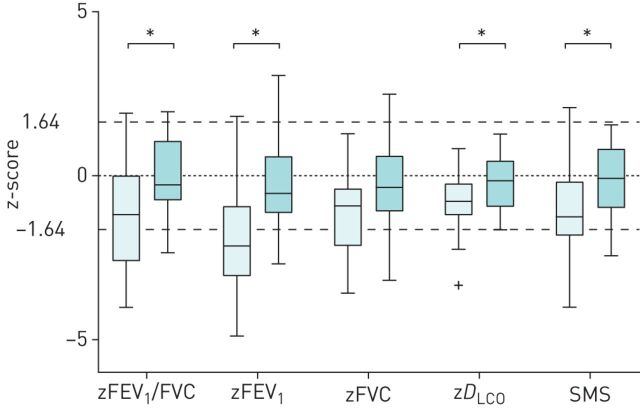
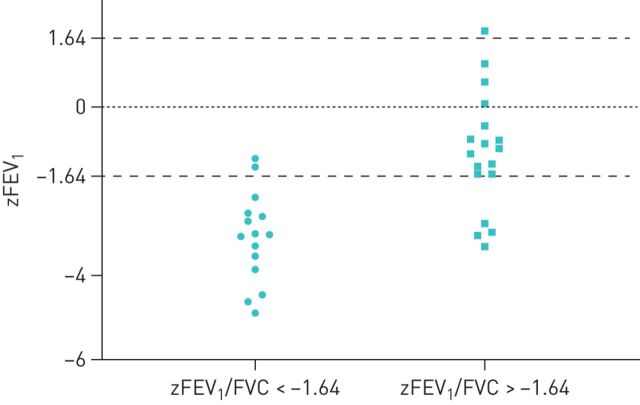
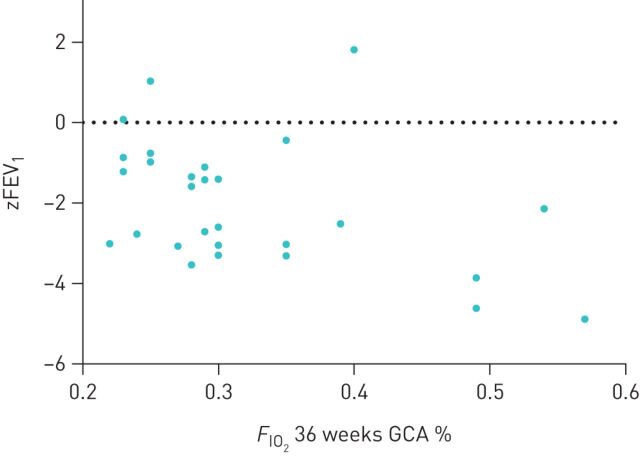
COPD risk is jointly determined by fetal lung development, lung growth rate and lung growth duration leading to the maximally attained level of lung function in early adulthood. Bronchopulmonary dysplasia (BPD) is considered a developmental arrest of alveolarisation. Long-term outcome studies of adult survivors born before the introduction of surfactant therapy ("old BPD") showed impaired lung function. We aimed to predict adult lung function and lung density in a cohort of premature infants born in the surfactant era, representing "new BPD". We studied a cohort of young adults born between 1987 and 1998, with (n=36) and without (n=28) BPD, treated in a single centre. Their perinatal characteristics and pulmonary function in infancy were studied by regression analysis for correlation with adult lung function and tissue lung density, all expressed by z-scores, at a mean age of 19.7±1.1 and 21±2.2 years, respectively. Although BPD adults had on average lower forced expiratory volume in 1 s (zFEV1)/forced vital capacity (FVC) and zFEV1 than those without, 55% of the BPD group had zFEV1/FVC values above the lower limit of normal (LLN). Moreover, above LLN values of diffusing capacity of the lung for carbon monoxide (zD LCO) was present in 89% of BPD adults and lung density in 71%. Only higher oxygen supply (F IO2) at 36 weeks post-conception of BPD subjects had a trend with lower zFEV1 (B=-6.4; p=0.053) and lower zD LCO (B=-4.1; p=0.023) at adulthood. No statistically significant predictors of new BPD were identified.
Copyright ©ERS 2020.
Conflict of interest statement
Conflict of interest: H.Y. Santema has nothing to disclose. Conflict of interest: J. Stolk has nothing to disclose. Conflict of interest: M. Los has nothing to disclose. Conflict of interest: B.C. Stoel has nothing to disclose. Conflict of interest: R. Tsonaka has nothing to disclose. Conflict of interest: I.T. Merth has nothing to disclose.
Figures
References
LinkOut - more resources
Full Text Sources