

Single rotation CTA of extracranial carotids integrated with cerebral CTP provides sufficient quality for decision making in patients with ischaemic stroke
- PMID: 33263488
- PMCID: PMC8041406
- DOI: 10.1177/1971400920974584
Single rotation CTA of extracranial carotids integrated with cerebral CTP provides sufficient quality for decision making in patients with ischaemic stroke
Abstract
Purpose: Large volume computed tomography scanners with 16 cm Z-axis single rotation coverage enable joggle-mode scanning of cerebral computed tomography perfusion and single rotation computed tomography angiography of cervical arteries. Our study aims to evaluate the feasibility of scanning cervical arteries, acquired with single rotation computed tomography angiography during computed tomography perfusion in ischaemic stroke patients.
Materials and methods: A total of 143 patients were scanned with a single contrast medium injection of 60 ml. Hounsfield units of the cervical arteries and veins were objectively measured and carotid bifurcations were subjectively reviewed. The incidence of artefacts and supra-aortic vessel coverage was recorded.
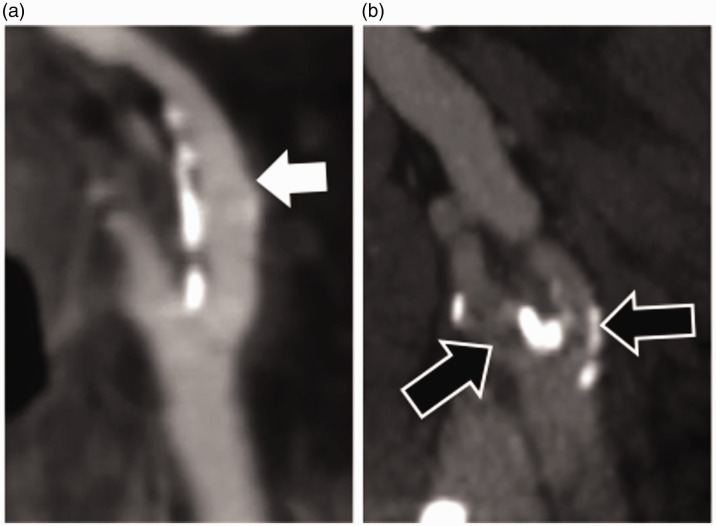
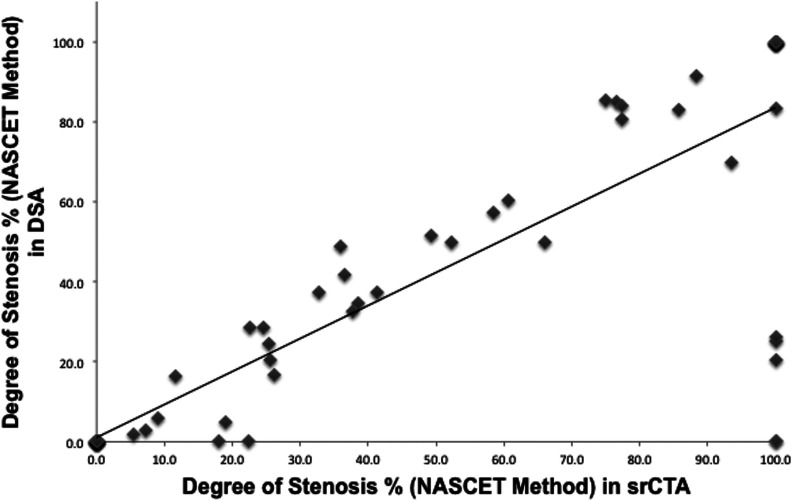
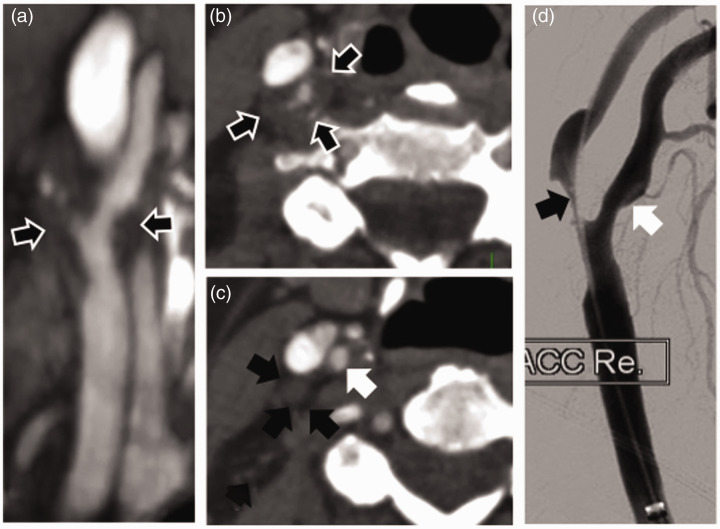
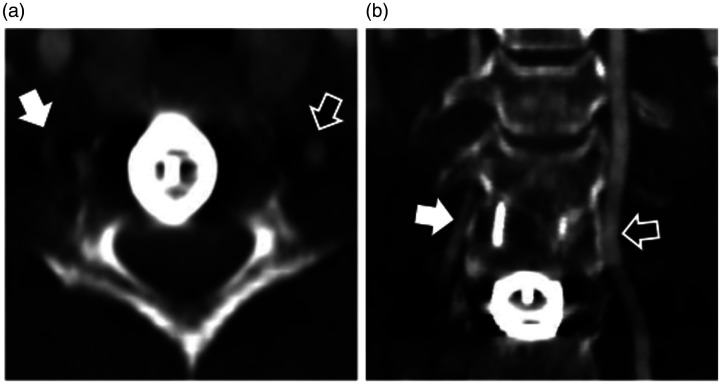
Results: Single rotation computed tomography angiography of the neck demonstrated supra-aortic vessels to their origins in 58 (40.6%) patients. Ninety-nine per cent (1140/1152) of arterial segments were adequately opacified (≥150 Hounsfield units). Arteries were adequately contrasted compared to veins in 81.3% (915/1126) of segments. However, the opacification was reversed in 14.0% (158/1126) of segments, indicating a delayed timing of acquisition; 95.5% (273/286) of carotid bifurcations were of good image quality. Measurement of internal carotid artery stenosis in single rotation computed tomography angiography according to the North American Symptomatic Carotid Endarterectomy Trial correlated well with digital subtraction angiography (R=0.87, P<0.05). Significant artefacts resulted from metal/dental implants (10.5%), contrast in central veins (7.7%) and the shoulder region (4.9%).
Conclusion: Single rotation computed tomography angiography of the neck incorporated into cerebral computed tomography perfusion with single contrast medium administration revealed adequate image quality for further decision-making in our patient sample. The main drawbacks were inadequate coverage of supra-aortic arteries and possible delay in timing of the joggle.
Keywords: Acute stroke imaging; computed tomography angiography; extracranial carotid arteries; joggle mode CT; one stop imaging; volume CT scanner.
Figures

Similar articles
-
Interleaving cerebral CT perfusion with neck CT angiography. Part II: clinical implementation and image quality.Eur Radiol. 2017 Jun;27(6):2411-2418. doi: 10.1007/s00330-016-4592-z. Epub 2016 Sep 21. Eur Radiol. 2017. PMID: 27651144 Free PMC article.
-
Modified Dual-Energy Algorithm for Calcified Plaque Removal: Evaluation in Carotid Computed Tomography Angiography and Comparison With Digital Subtraction Angiography.Invest Radiol. 2017 Nov;52(11):680-685. doi: 10.1097/RLI.0000000000000391. Invest Radiol. 2017. PMID: 28542096
-
Sixty-four-section multidetector CT angiography of carotid arteries: a systematic analysis of image quality and artifacts.AJNR Am J Neuroradiol. 2010 Jan;31(1):91-9. doi: 10.3174/ajnr.A1768. Epub 2009 Sep 3. AJNR Am J Neuroradiol. 2010. PMID: 19729539 Free PMC article.
-
Non-invasive assessment of neck-vessel pathology.Eur Radiol. 1998;8(5):691-7. doi: 10.1007/s003300050461. Eur Radiol. 1998. PMID: 9601954 Review.
-
Imaging spectrum of extracranial arterial vascular pathology: pearls for the radiologist.Clin Radiol. 2022 Mar;77(3):167-178. doi: 10.1016/j.crad.2021.10.011. Epub 2021 Nov 17. Clin Radiol. 2022. PMID: 34799048 Review.
References
-
- Garg N, Eshkar N, Tanenbaum L, et al.. Computed tomography angiographic correlates of early computed tomography signs in acute ischemic stroke. J Neuroimaging Off J Am Soc Neuroimaging 2004; 14: 242–245. - PubMed
-
- Ezzeddine MA, Lev MH, McDonald CT, et al.. CT angiography with whole brain perfused blood volume imaging: added clinical value in the assessment of acute stroke. Stroke J Cereb Circ 2002; 33: 959–966. - PubMed
-
- Scaroni R, Tambasco N, Cardaioli G, et al.. Multimodal use of computed tomography in early acute stroke, part 2. Clin Exp Hypertens N Y N 1993 2006; 28: 427–431. - PubMed
-
- Zhu G, Michel P, Aghaebrahim A, et al.. Computed tomography workup of patients suspected of acute ischemic stroke: perfusion computed tomography adds value compared with clinical evaluation, non-contrast computed tomography, and computed tomography angiogram in terms of predicting outcome. Stroke J Cereb Circ 2013; 44: 1049–1055. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
