

Clinicopathological Analysis of Acute/Active Antibody-Mediated Rejection in Renal Allografts According to the Banff 2013 Classification
- PMID: 33264791
- PMCID: PMC7949198
- DOI: 10.1159/000512143
Clinicopathological Analysis of Acute/Active Antibody-Mediated Rejection in Renal Allografts According to the Banff 2013 Classification
Abstract
Aim: This study evaluated the clinicopathological findings of acute/active antibody-mediated rejection (AABMR) according to the Banff 2013 classification.
Methods: We analyzed 345 biopsies of 269 kidney transplant recipients. Pathological AABMR (PAABMR) was defined as histological evidence of acute tissue injury and endothelial injury by light microscopy regardless of donor-specific antibodies (DSAs).
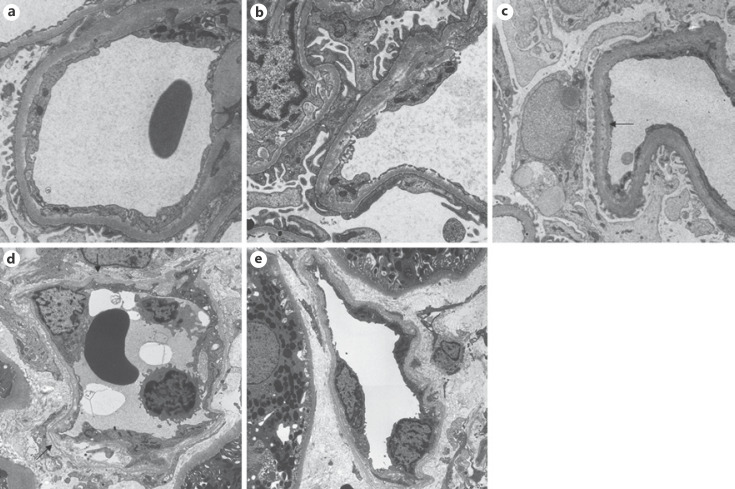
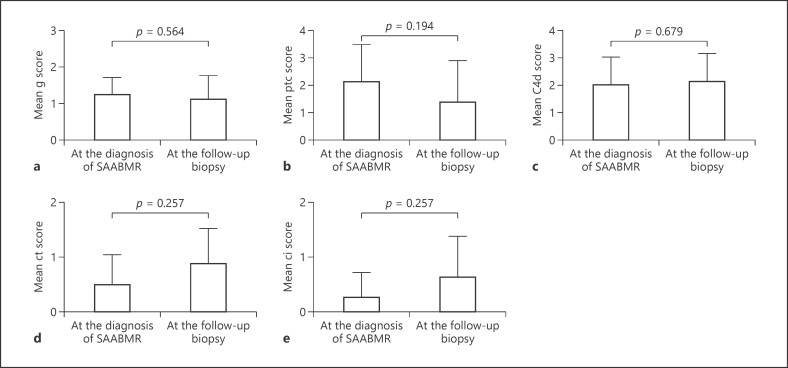
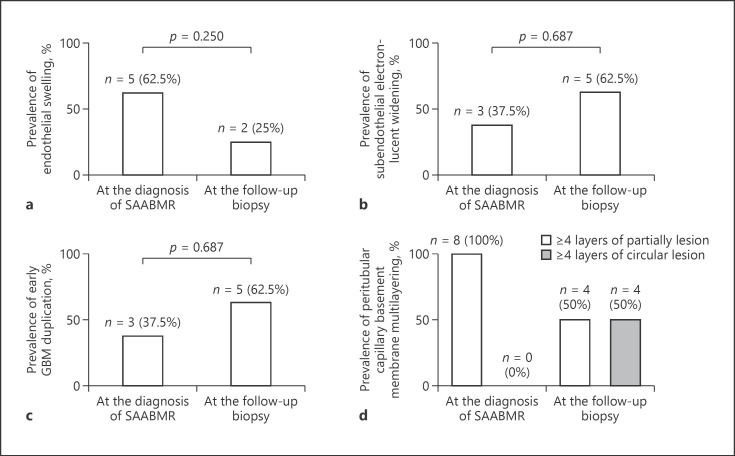
Results: Among the 345 biopsies, 29 (8.4%) were diagnosed as PAABMR. The mean g score was 1.17 ± 0.60, the mean ptc score was 1.97 ± 1.32, and DSA positivity was found in 69% of PAABMR. The mean duration after transplantation was 22.9 ± 26.7 months. Among 3 groups (DSA-high, mean fluorescence intensity (MFI) ≥ 5,000; DSA-low, MFI < 5,000 to ≥1,000; below cutoff), ABO incompatibility in DSA-high was significantly lower and second transplantation in DSA-high was significantly higher. We found 83% of PAABMR by the protocol biopsy (subclinical AABMR [SAABMR]). The short-term clinical and light microscopical changes in 8 cases of SAABMR did not show worsening during follow-up period (9-24 months). However, ultrastructural finding, including glomerular endothelial swelling, subendothelial electron-lucent widening, and early glomerular basement duplication, were found by electron microscopy (EM) in the first biopsies, and half of the SAABMR cases developed de novo circular peritubular capillary multilayering in the follow-up biopsies.
Conclusion: PAABMR was mainly found by the protocol biopsy. The short-term follow-up of SAABMR patients did not show worsening clinically and light microscopically, but ultrastructural examination by EM was useful to detect early lesions of endothelial injury and progression of glomerular and peritubular capillary basement membrane alterations.
Keywords: Acute/active antibody-mediated rejection; Allograft; Banff 2013 classification; Electron microscopy; Kidney transplantation.
© 2020 The Author(s) Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Haas M, Sis B, Racusen LC, Solez K, Glotz D, Colvin RB, et al. Banff 2013 meeting report: inclusion of c4d-negative antibody-mediated rejection and antibody-associated arterial lesions. Am J Transplant. 2014;14((2)):272–83. - PubMed
-
- Haas M, Mirocha J. Early ultrastructural changes in renal allografts: correlation with antibody-mediated rejection and transplant glomerulopathy. Am J Transplant. 2011 Oct;11((10)):2123–31. - PubMed
-
- Eskandary F, Bond G, Kozakowski N, Regele H, Marinova L, Wahrmann M, et al. Diagnostic contribution of donor-specific antibody characteristics to uncover late silent antibody-mediated rejection-results of a cross-sectional screening study. Transplantation. 2017;101((3)):631–41. - PubMed
-
- Wavamunno MD, O'Connell PJ, Vitalone M, Fung CL, Allen RD, Chapman JR, et al. Transplant glomerulopathy: ultrastructural abnormalities occur early in longitudinal analysis of protocol biopsies. Am J Transplant. 2007;7((12)):2757–68. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
