

Current understanding of primary biliary cholangitis
- PMID: 33264835
- PMCID: PMC7820210
- DOI: 10.3350/cmh.2020.0028
Current understanding of primary biliary cholangitis
Abstract
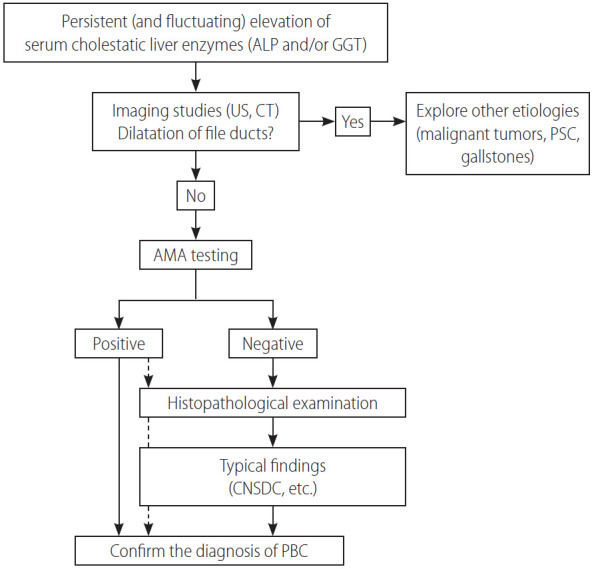
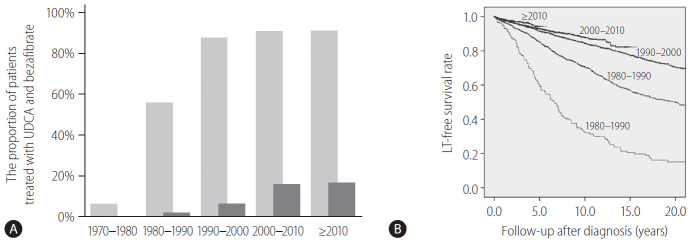
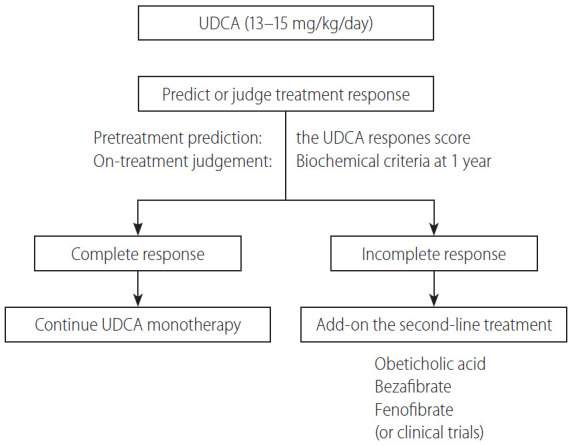
Primary biliary cholangitis (PBC) causes chronic and persistent cholestasis in the liver, eventually resulting in cirrhosis and hepatic failure without appropriate treatment. PBC mainly develops in middle-aged women, but it is also common in young women and men. PBC is considered a model of autoimmune disease because of the presence of diseasespecific autoantibodies, that is, antimitochondrial antibodies (AMAs), intense infiltration of mononuclear cells into the bile ducts, and a high prevalence of autoimmune diseases such as comorbidities. Histologically, PBC is characterized by degeneration and necrosis of intrahepatic biliary epithelial cells surrounded by a dense infiltration of mononuclear cells, coined as chronic non-suppurative destructive cholangitis, which leads to destructive changes and the disappearance of small- or medium-sized bile ducts. Since 1990, early diagnosis with the detection of AMAs and introduction of ursodeoxycholic acid as first-line treatment has greatly altered the clinical course of PBC, and liver transplantation-free survival of patients with PBC is now comparable to that of the general population.
Keywords: Anti-mitochondrial antibody; Bezafibrate; Epidemiology.
Conflict of interest statement
Figures

Comment in
-
Clinical and serological prognostic markers in primary biliary cholangitis.Clin Mol Hepatol. 2021 Apr;27(2):360-361. doi: 10.3350/cmh.2021.0088. Epub 2021 Mar 23. Clin Mol Hepatol. 2021. PMID: 33752318 Free PMC article. No abstract available.
References
-
- Addison T, Gull W. On a certain affection of the skin-vitiligoidea-alpha-plana, B-tuberosa. Guys Hosp Rep. 1851;7:265–276.
-
- Beuers U, Gershwin ME, Gish RG, Invernizzi P, Jones DE, Lindor K, et al. Changing nomenclature for PBC: from ‘cirrhosis’ to ‘cholangitis’. Clin Res Hepatol Gastroenterol. 2015;39:e57–e59. - PubMed
-
- Beuers U, Gershwin ME, Gish RG, Invernizzi P, Jones DE, Lindor K, et al. Changing nomenclature for PBC: from ‘cirrhosis’ to ‘cholangitis’. Dig Liver Dis. 2015;47:924–926. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
