

Xanthine Oxidase Drives Hemolysis and Vascular Malfunction in Sickle Cell Disease
- PMID: 33267657
- PMCID: PMC8185582
- DOI: 10.1161/ATVBAHA.120.315081
Xanthine Oxidase Drives Hemolysis and Vascular Malfunction in Sickle Cell Disease
Abstract
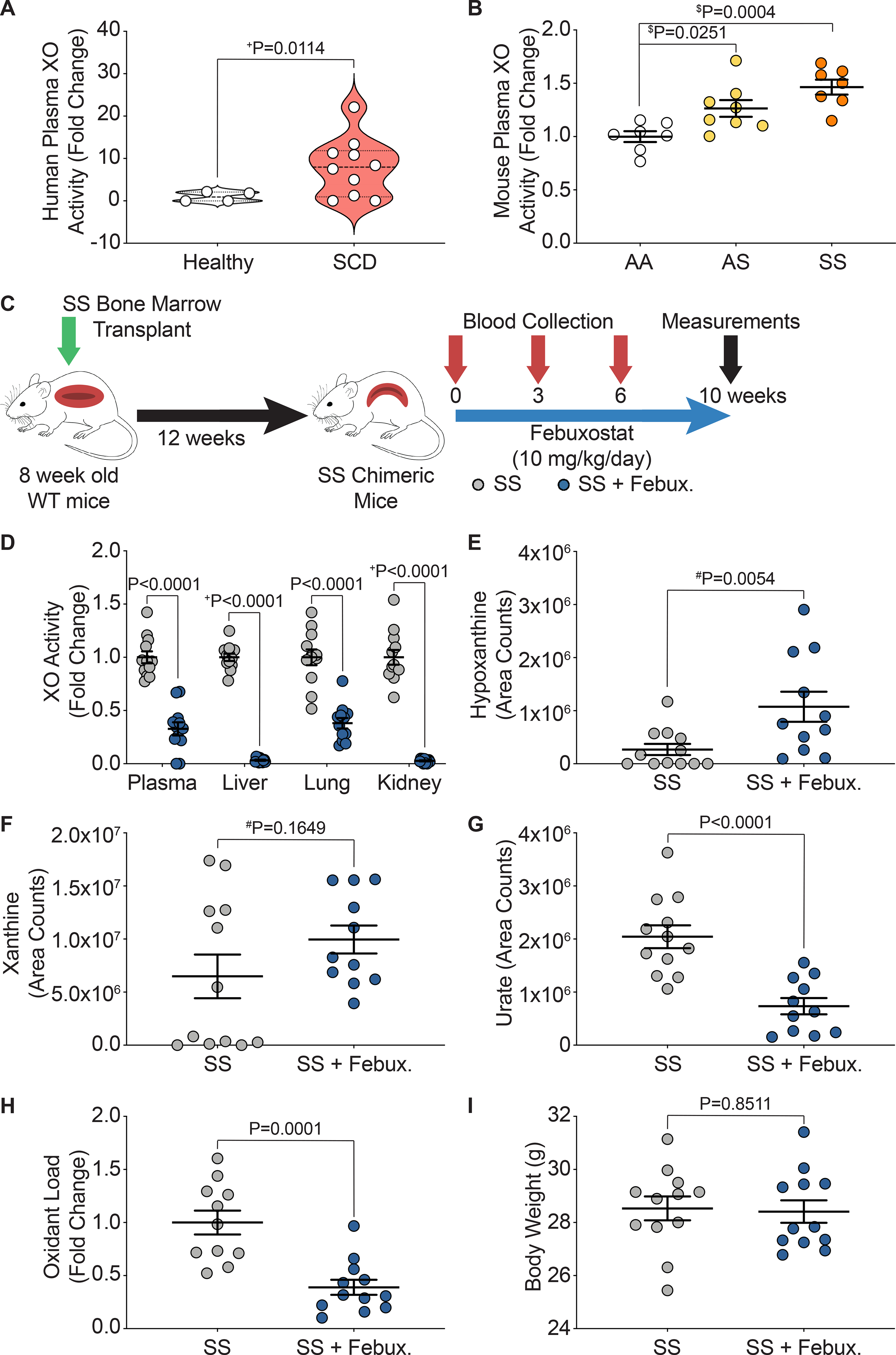
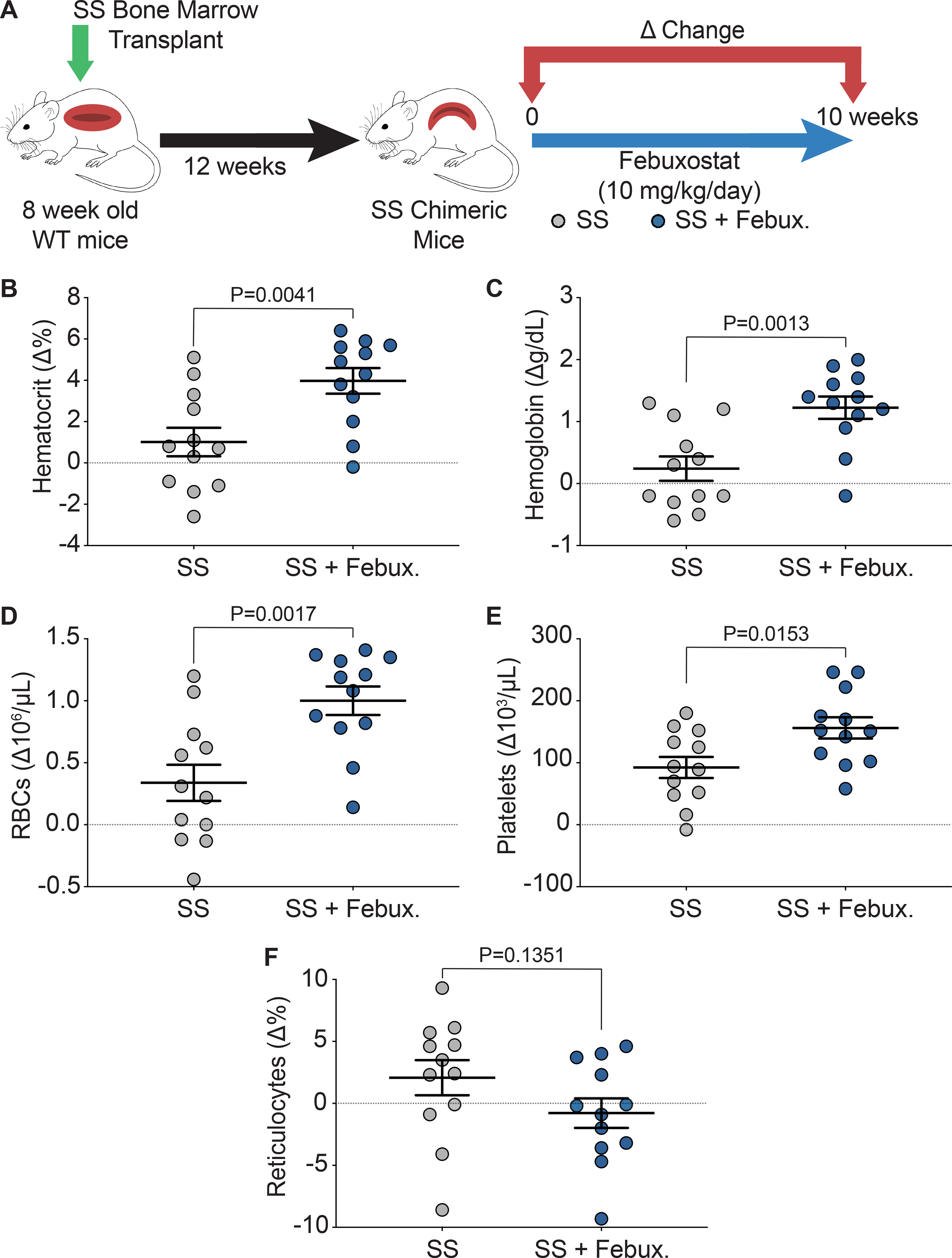
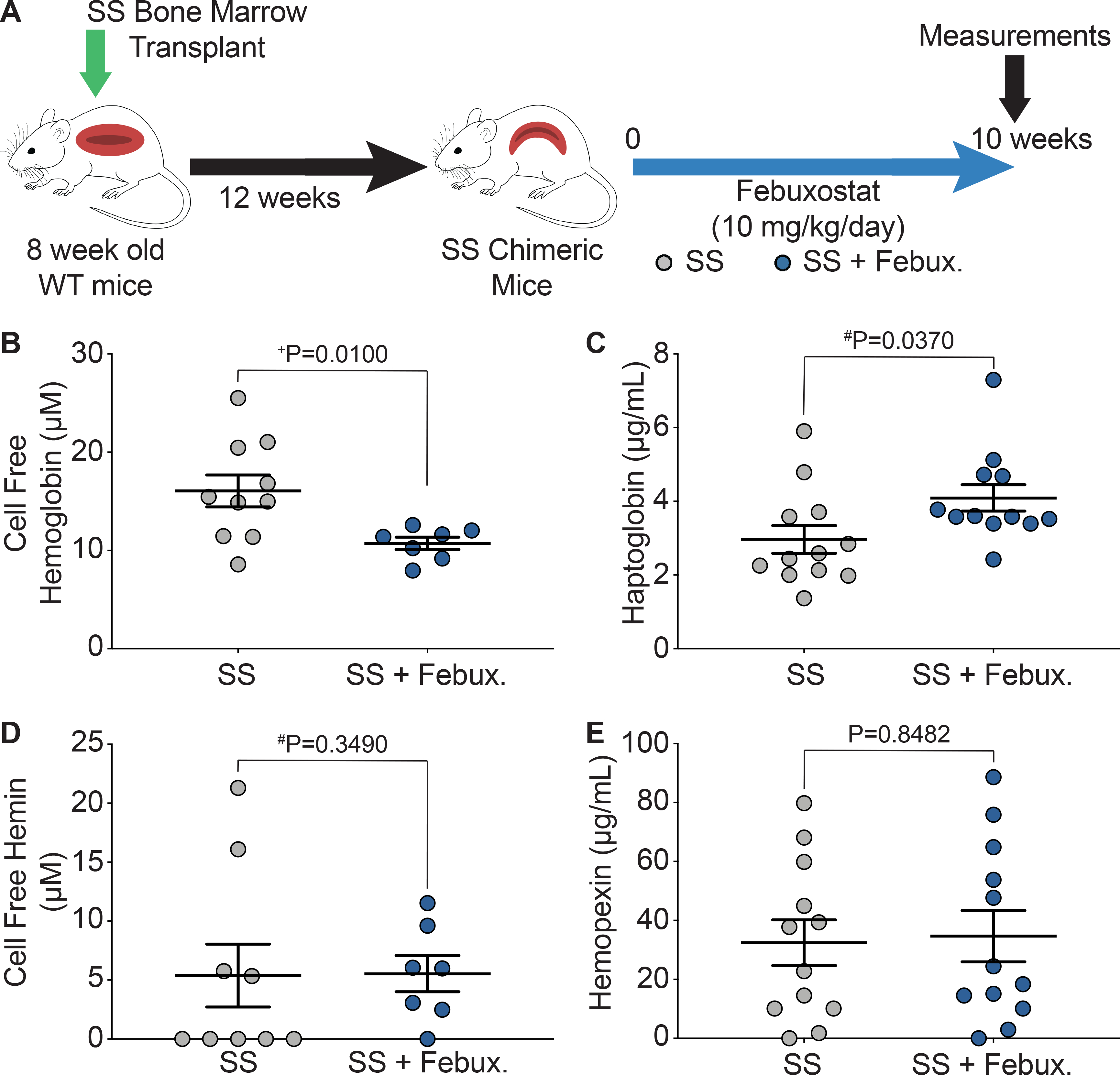
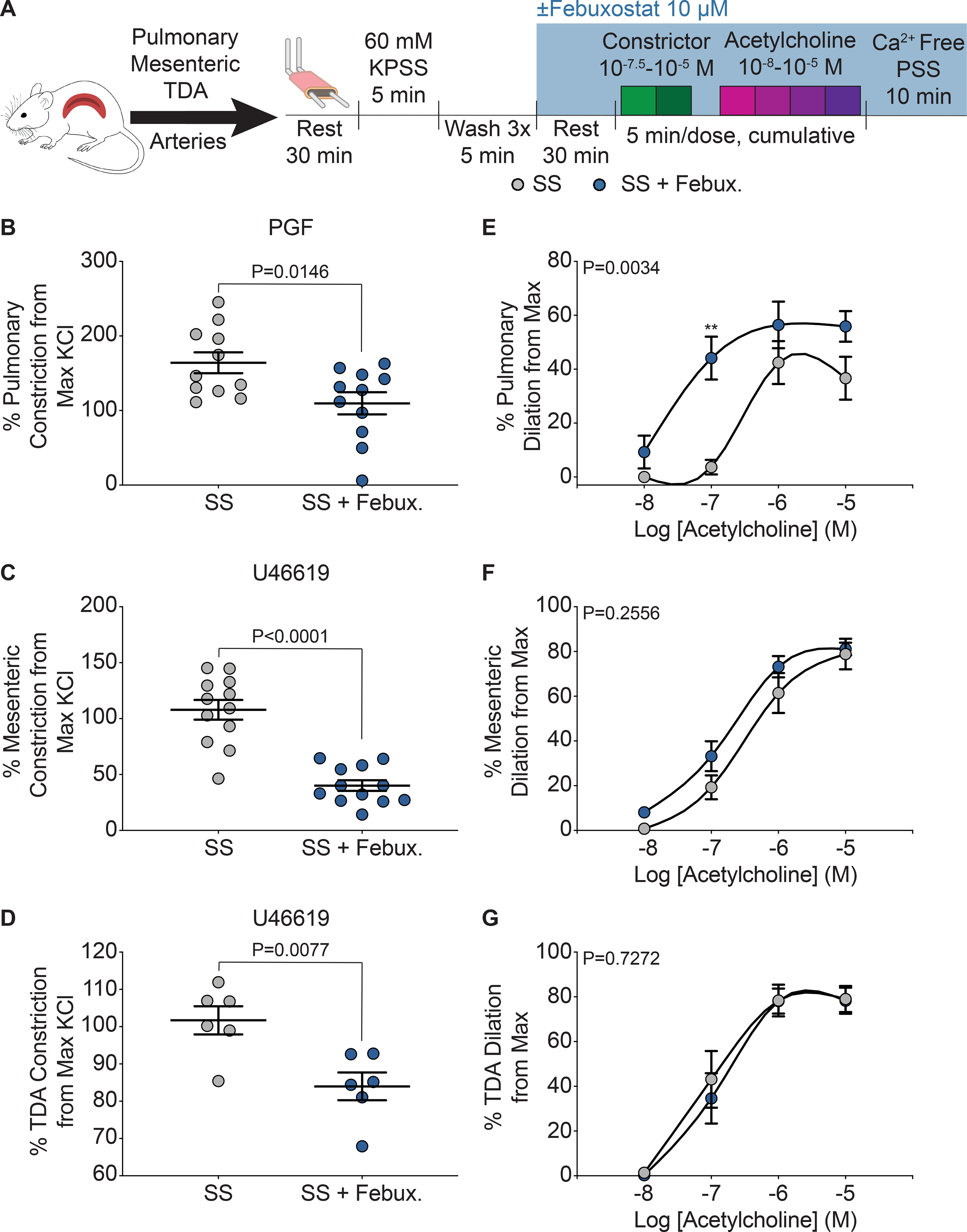
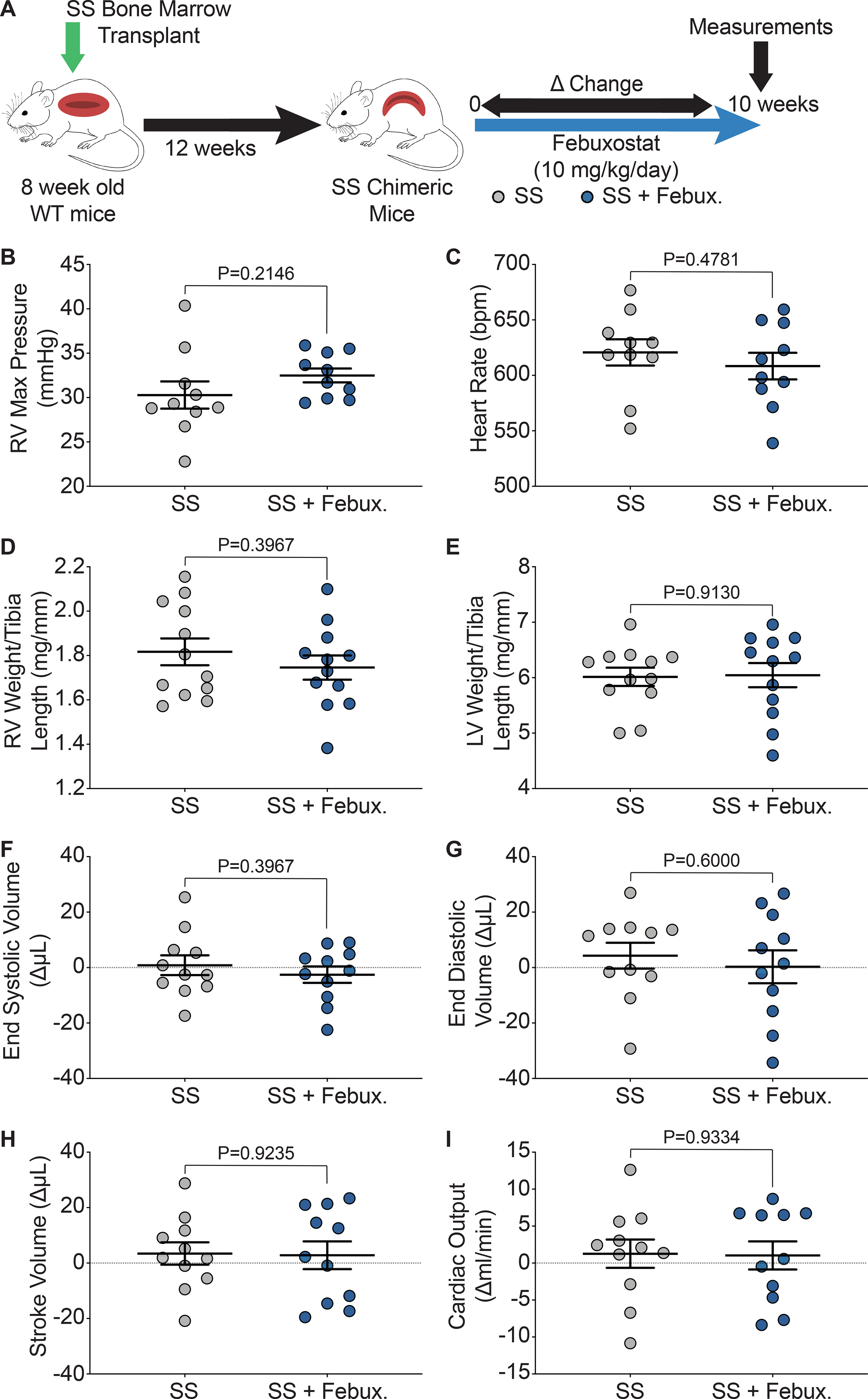
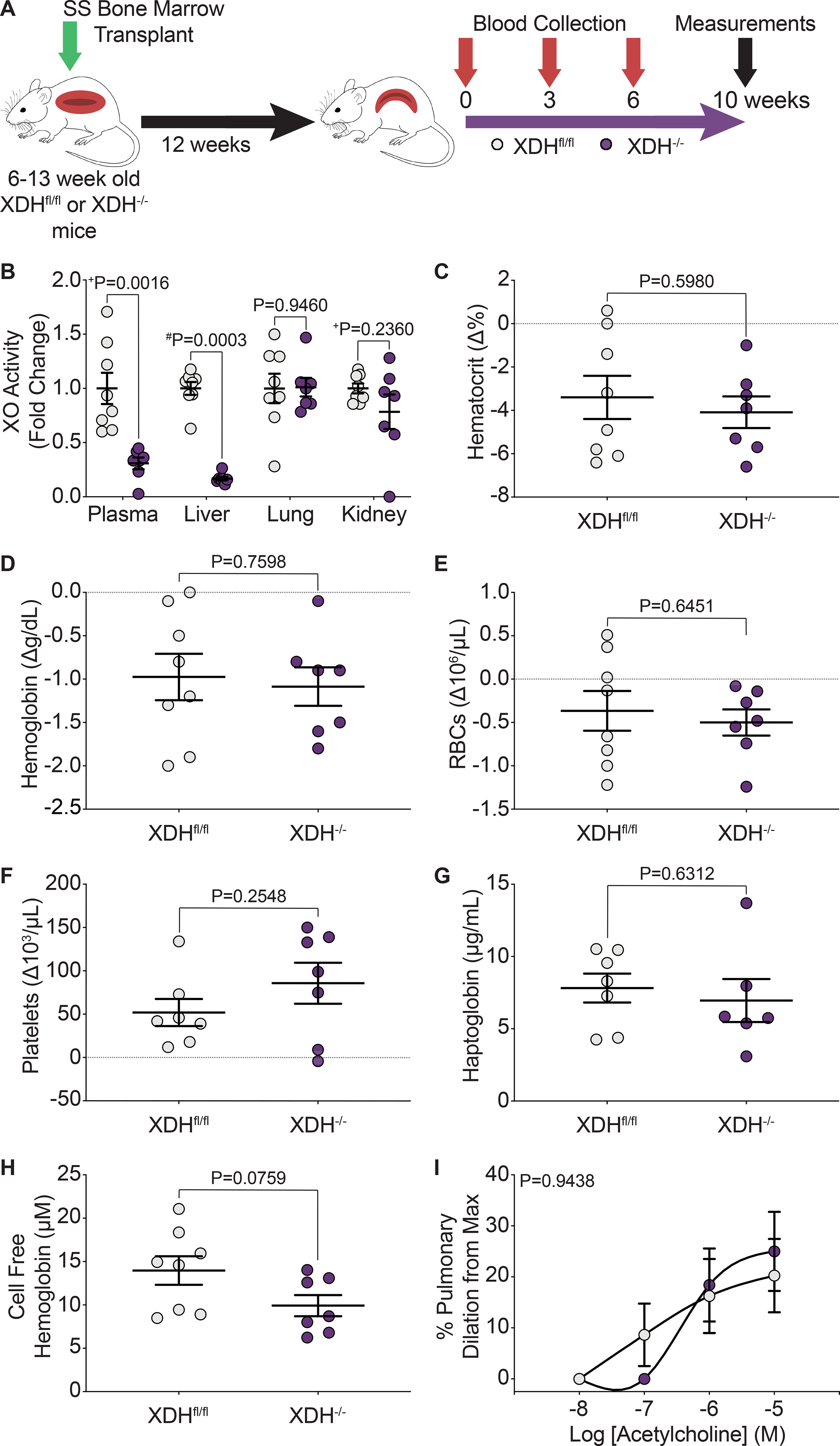
Objective: Chronic hemolysis is a hallmark of sickle cell disease (SCD) and a driver of vasculopathy; however, the mechanisms contributing to hemolysis remain incompletely understood. Although XO (xanthine oxidase) activity has been shown to be elevated in SCD, its role remains unknown. XO binds endothelium and generates oxidants as a byproduct of hypoxanthine and xanthine catabolism. We hypothesized that XO inhibition decreases oxidant production leading to less hemolysis. Approach and Results: Wild-type mice were bone marrow transplanted with control (AA) or sickle (SS) Townes bone marrow. After 12 weeks, mice were treated with 10 mg/kg per day of febuxostat (Uloric), Food and Drug Administration-approved XO inhibitor, for 10 weeks. Hematologic analysis demonstrated increased hematocrit, cellular hemoglobin, and red blood cells, with no change in reticulocyte percentage. Significant decreases in cell-free hemoglobin and increases in haptoglobin suggest XO inhibition decreased hemolysis. Myographic studies demonstrated improved pulmonary vascular dilation and blunted constriction, indicating improved pulmonary vasoreactivity, whereas pulmonary pressure and cardiac function were unaffected. The role of hepatic XO in SCD was evaluated by bone marrow transplanting hepatocyte-specific XO knockout mice with SS Townes bone marrow. However, hepatocyte-specific XO knockout, which results in >50% diminution in circulating XO, did not affect hemolysis levels or vascular function, suggesting hepatocyte-derived elevation of circulating XO is not the driver of hemolysis in SCD.
Conclusions: Ten weeks of febuxostat treatment significantly decreased hemolysis and improved pulmonary vasoreactivity in a mouse model of SCD. Although hepatic XO accounts for >50% of circulating XO, it is not the source of XO driving hemolysis in SCD.
Keywords: anemia, sickle cell; bone marrow; endothelium; febuxostat; hemolysis; xanthine oxidase.
Figures
Similar articles
-
Release of hepatic xanthine oxidase (XO) to the circulation is protective in intravascular hemolytic crisis.Redox Biol. 2023 Jun;62:102636. doi: 10.1016/j.redox.2023.102636. Epub 2023 Feb 13. Redox Biol. 2023. PMID: 36906950 Free PMC article.
-
Febuxostat, a novel xanthine oxidoreductase inhibitor, improves hypertension and endothelial dysfunction in spontaneously hypertensive rats.Naunyn Schmiedebergs Arch Pharmacol. 2016 Aug;389(8):831-8. doi: 10.1007/s00210-016-1239-1. Epub 2016 May 20. Naunyn Schmiedebergs Arch Pharmacol. 2016. PMID: 27198514 Free PMC article.
-
The impact of xanthine oxidase (XO) on hemolytic diseases.Redox Biol. 2019 Feb;21:101072. doi: 10.1016/j.redox.2018.101072. Epub 2018 Dec 10. Redox Biol. 2019. PMID: 30580157 Free PMC article. Review.
-
Inhibition of xanthine oxidase in the acute phase of myocardial infarction prevents skeletal muscle abnormalities and exercise intolerance.Cardiovasc Res. 2021 Feb 22;117(3):805-819. doi: 10.1093/cvr/cvaa127. Cardiovasc Res. 2021. PMID: 32402072
-
Xanthine oxidase inhibitors beyond allopurinol and febuxostat; an overview and selection of potential leads based on in silico calculated physico-chemical properties, predicted pharmacokinetics and toxicity.Eur J Med Chem. 2017 Jul 28;135:491-516. doi: 10.1016/j.ejmech.2017.04.031. Epub 2017 Apr 19. Eur J Med Chem. 2017. PMID: 28478180 Review.
Cited by
-
Cooperation between CYB5R3 and NOX4 via coenzyme Q mitigates endothelial inflammation.Redox Biol. 2021 Nov;47:102166. doi: 10.1016/j.redox.2021.102166. Epub 2021 Oct 14. Redox Biol. 2021. PMID: 34656824 Free PMC article.
-
Xanthine oxidase levels and immune dysregulation are independently associated with anemia in Plasmodium falciparum malaria.Sci Rep. 2023 Sep 7;13(1):14720. doi: 10.1038/s41598-023-41764-4. Sci Rep. 2023. PMID: 37679382 Free PMC article.
-
Endothelial superoxide dismutase 2 is decreased in sickle cell disease and regulates fibronectin processing.Function (Oxf). 2022 Feb 17;3(2):zqac005. doi: 10.1093/function/zqac005. eCollection 2022. Function (Oxf). 2022. PMID: 35274104 Free PMC article.
-
Liquid chromatography coupled to mass spectrometry metabolomic analysis of cerebrospinal fluid revealed the metabolic characteristics of moyamoya disease.Front Neurol. 2024 Feb 15;15:1298385. doi: 10.3389/fneur.2024.1298385. eCollection 2024. Front Neurol. 2024. PMID: 38426176 Free PMC article.
-
The oral ferroportin inhibitor vamifeport improves hemodynamics in a mouse model of sickle cell disease.Blood. 2022 Aug 18;140(7):769-781. doi: 10.1182/blood.2021014716. Blood. 2022. PMID: 35714304 Free PMC article.
References
-
- Pinto VM, Balocco M, Quintino S and Forni GL. Sickle cell disease: a review for the internist. Intern Emerg Med. 2019;14:1051–1064. - PubMed
-
- Kato GJ, Piel FB, Reid CD, Gaston MH, Ohene-Frempong K, Krishnamurti L, Smith WR, Panepinto JA, Weatherall DJ, Costa FF and Vichinsky EP. Sickle cell disease. Nat Rev Dis Primers. 2018;4:18010. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
