

Association between biomarkers and COVID-19 severity and mortality: a nationwide Danish cohort study
- PMID: 33268425
- PMCID: PMC7712929
- DOI: 10.1136/bmjopen-2020-041295
Association between biomarkers and COVID-19 severity and mortality: a nationwide Danish cohort study
Abstract
Objective: To evaluate the association between common biomarkers, death and intensive care unit (ICU) admission in patients with COVID-19.
Design: Retrospective cohort study. From electronic national registry data, we used Cox analysis and bootstrapping to evaluate associations between baseline levels of biomarkers and standardised absolute risks of death/ICU admission, adjusted for age and gender.
Setting: All hospitals in Denmark.
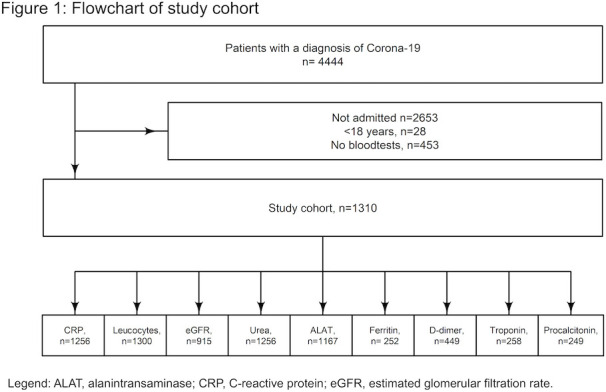
Participants: 1310 patients aged ≥18 years admitted to hospital with COVID-19 from 27th of February to 1st of May 2020, with available biochemistry data.
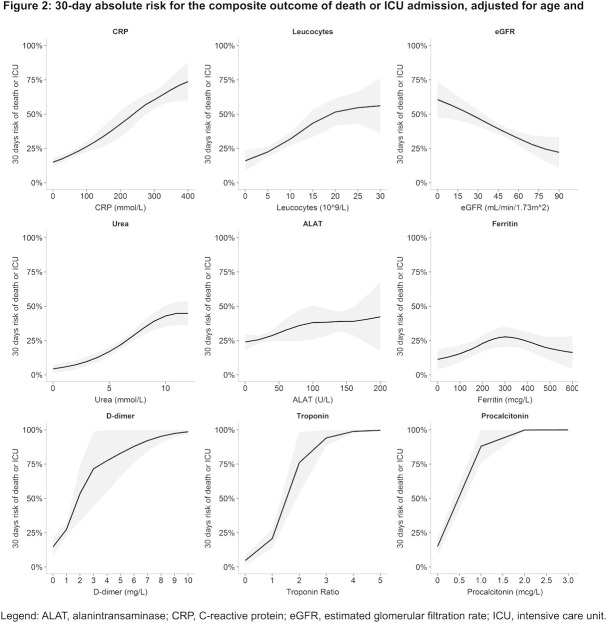
Main outcome measures: A composite of death/ICU admission occurring within 30 days.
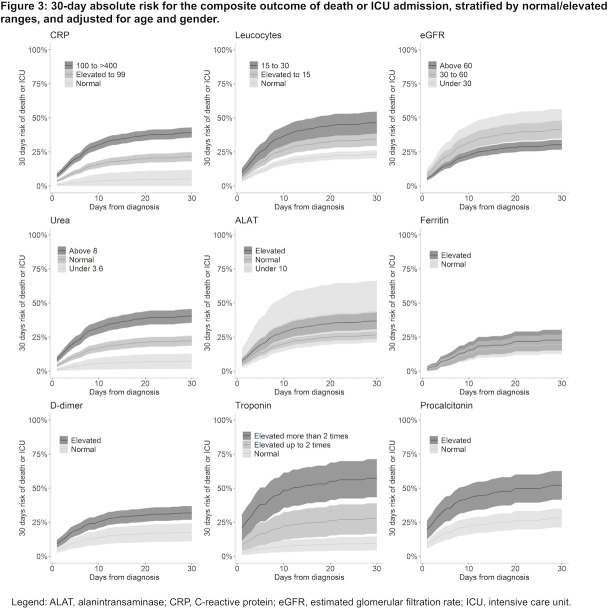
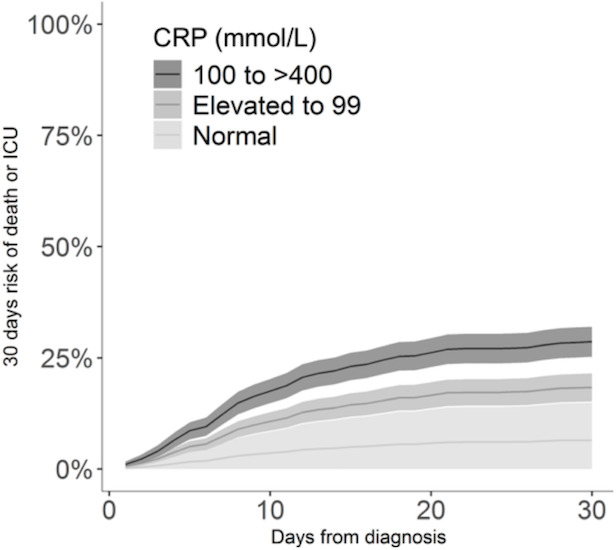
Results: Of the 1310 patients admitted to hospital (54.6% men; median age 73.6 years), 352 (26.9%) experienced the composite endpoint and 263 (20.1%) died. For the composite endpoint, the absolute risks for moderately and severely elevated C reactive protein (CRP) were significantly higher, 21.5% and 39.2%, respectively, compared with 5.0% for those with normal CRP. Moderately and severely elevated leucocytes were significantly higher, 34.5% and 46.6% risk, respectively, compared with 23.2% for those with normal leucocytes. Moderately and severely decreased estimated glomerular filtration rates (eGFR) were significantly higher, 41.5% and 45.9% risk, respectively, compared with 30.4% for those with normal/mildly decreased eGFR. Normal and elevated ureas were significantly higher, 22.3% and 40.6% risk, respectively, compared with 7.3% for those with low urea. Elevated D-dimer was significantly higher, 31.8% risk, compared with 17.5% for those with normal D-dimer. Moderately and severely elevated troponins were significantly higher, 27.7% and 57.3% risk, respectively, compared with 9.4% for those with normal troponin. Elevated procalcitonin was significantly higher, 52.1% risk, compared with 28.0% for those with normal procalcitonin.
Conclusion: In this nationwide study of patients admitted with COVID-19, elevated levels of CRP, leucocytes, procalcitonin, urea, troponins and D-dimer, and low levels of eGFR were associated with higher standardised absolute risk of death/ICU admission within 30 days.
Keywords: adult intensive & critical care; general medicine (see internal medicine); infectious diseases.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization Coronavirus disease (COVID-19) outbreak. Available: https://www.who.int
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous