

The effect of semaglutide 2.4 mg once weekly on energy intake, appetite, control of eating, and gastric emptying in adults with obesity
- PMID: 33269530
- PMCID: PMC7898914
- DOI: 10.1111/dom.14280
The effect of semaglutide 2.4 mg once weekly on energy intake, appetite, control of eating, and gastric emptying in adults with obesity
Abstract
Aim: To investigate the effects of once-weekly subcutaneous (s.c.) semaglutide 2.4 mg on gastric emptying, appetite, and energy intake in adults with obesity.
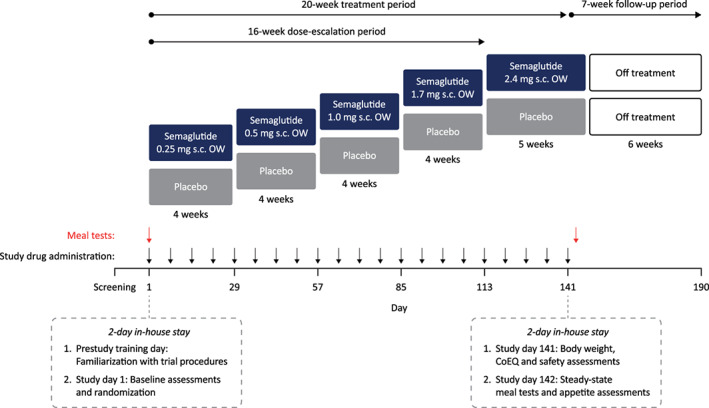
Materials and methods: A double-blind, parallel-group trial was conducted in 72 adults with obesity, randomized to once-weekly s.c. semaglutide (dose-escalated to 2.4 mg) or placebo for 20 weeks. Gastric emptying was assessed using paracetamol absorption following a standardized breakfast. Participant-reported appetite ratings and Control of Eating Questionnaire (CoEQ) responses were assessed, and energy intake was measured during ad libitum lunch.
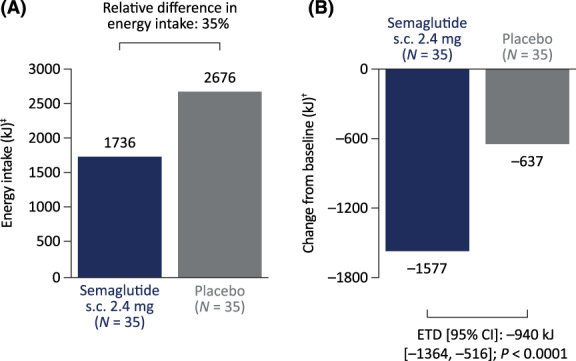
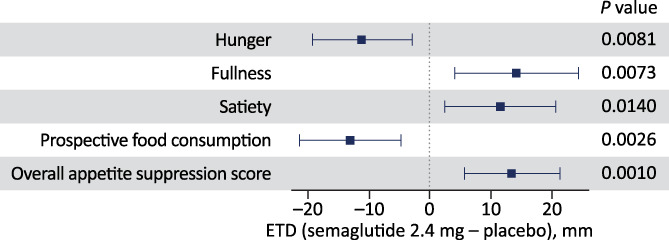
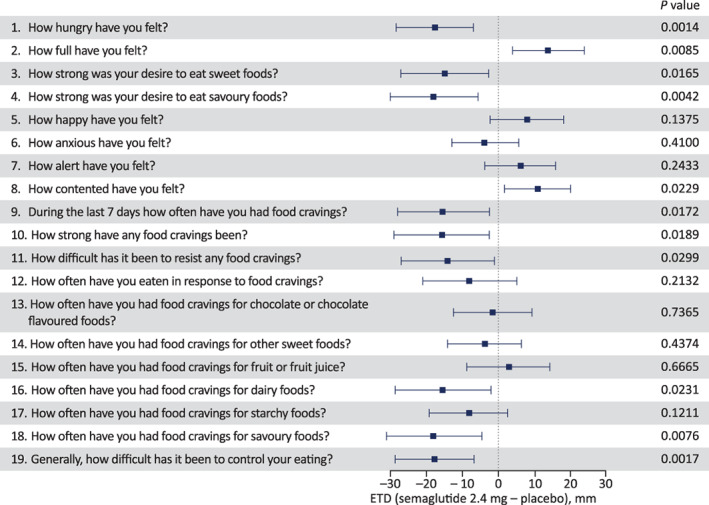
Results: The area under the concentration-time curve (AUC) for paracetamol 0 to 5 hours after a standardized meal (AUC0-5h,para ; primary endpoint) was increased by 8% (P = 0.005) with semaglutide 2.4 mg versus placebo at week 20 (non-significant when corrected for week 20 body weight; P = 0.12). No effect was seen on AUC0-1h,para , maximum observed paracetamol concentration, or time to maximum observed paracetamol concentration. Ad libitum energy intake was 35% lower with semaglutide versus placebo (1736 versus 2676 kJ; estimated treatment difference -940 kJ; P <0.0001). Semaglutide reduced hunger and prospective food consumption, and increased fullness and satiety when compared with placebo (all P <0.02). The CoEQ indicated better control of eating and fewer/weaker food cravings with semaglutide versus placebo (P <0.05). Body weight was reduced by 9.9% with semaglutide and 0.4% with placebo. Safety was consistent with the known profile of semaglutide.
Conclusions: In adults with obesity, once-weekly s.c. semaglutide 2.4 mg suppressed appetite, improved control of eating, and reduced food cravings, ad libitum energy intake and body weight versus placebo. There was no evidence of delayed gastric emptying at week 20, assessed indirectly via paracetamol absorption.
Keywords: GLP-1 analogue; appetite; control of eating; energy intake; food craving; gastric emptying; glucagon-like peptide-1; obesity; randomized trial; semaglutide.
© 2020 The Authors. Diabetes, Obesity and Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
M.F., S.T. and D.S. are employees and shareholders of Novo Nordisk, the sponsor of this trial; A.W. is an employee of Novo Nordisk. A.B. is an employee of Parexel International GmbH; Parexel International GmbH was paid by Novo Nordisk for assistance in conducting the study.
Figures
References
-
- Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(Suppl 3):1‐203. - PubMed
-
- American Diabetes Association . 8. Obesity management for the treatment of type 2 diabetes: standards of medical care in diabetes‐2020. Diabetes Care. 2020;43(Suppl 1):S89‐S97. [Addendum: Diabetes Care. 2020;43(8):1980‐1980]. - PubMed
-
- Nauck MA, Meier JJ. Are all GLP‐1 agonists equal in the treatment of type 2 diabetes? Eur J Endocrinol. 2019;181(6):R211‐R234. - PubMed
-
- O'Neil PM, Birkenfeld AL, McGowan B, et al. Efficacy and safety of semaglutide compared with liraglutide and placebo for weight loss in patients with obesity: a randomised, double‐blind, placebo and active controlled, dose‐ranging, phase 2 trial. Lancet. 2018;392(10148):637‐649. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
