

Number of Social Determinants of Health and Fatal and Nonfatal Incident Coronary Heart Disease in the REGARDS Study
- PMID: 33269599
- PMCID: PMC7856168
- DOI: 10.1161/CIRCULATIONAHA.120.048026
Number of Social Determinants of Health and Fatal and Nonfatal Incident Coronary Heart Disease in the REGARDS Study
Abstract
Background: Social determinants of health (SDH) are individually associated with incident coronary heart disease (CHD) events. Indices reflecting social deprivation have been developed for population management, but are difficult to operationalize during clinical care. We examined whether a simple count of SDH is associated with fatal incident CHD and nonfatal myocardial infarction (MI).
Methods: We used data from the prospective longitudinal REGARDS cohort study (Reasons for Geographic and Racial Differences in Stroke), a national population-based sample of community-dwelling Black and White adults age ≥45 years recruited from 2003 to 2007. Seven SDH from the 5 Healthy People 2020 domains included social context (Black race, social isolation); education (educational attainment); economic stability (annual household income); neighborhood (living in a zip code with high poverty); and health care (lacking health insurance, living in 1 of the 9 US states with the least public health infrastructure). Outcomes were expert adjudicated fatal incident CHD and nonfatal MI.
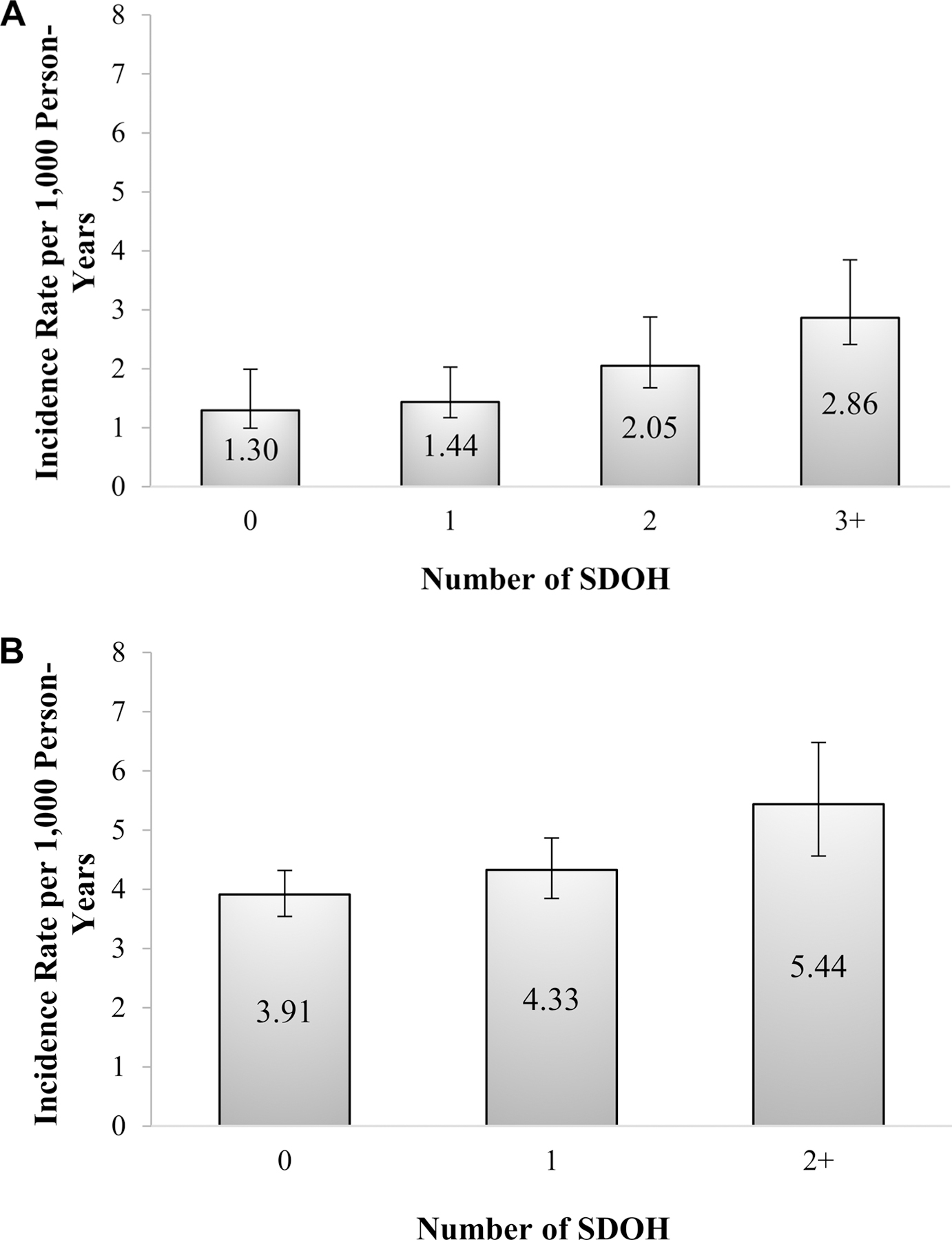
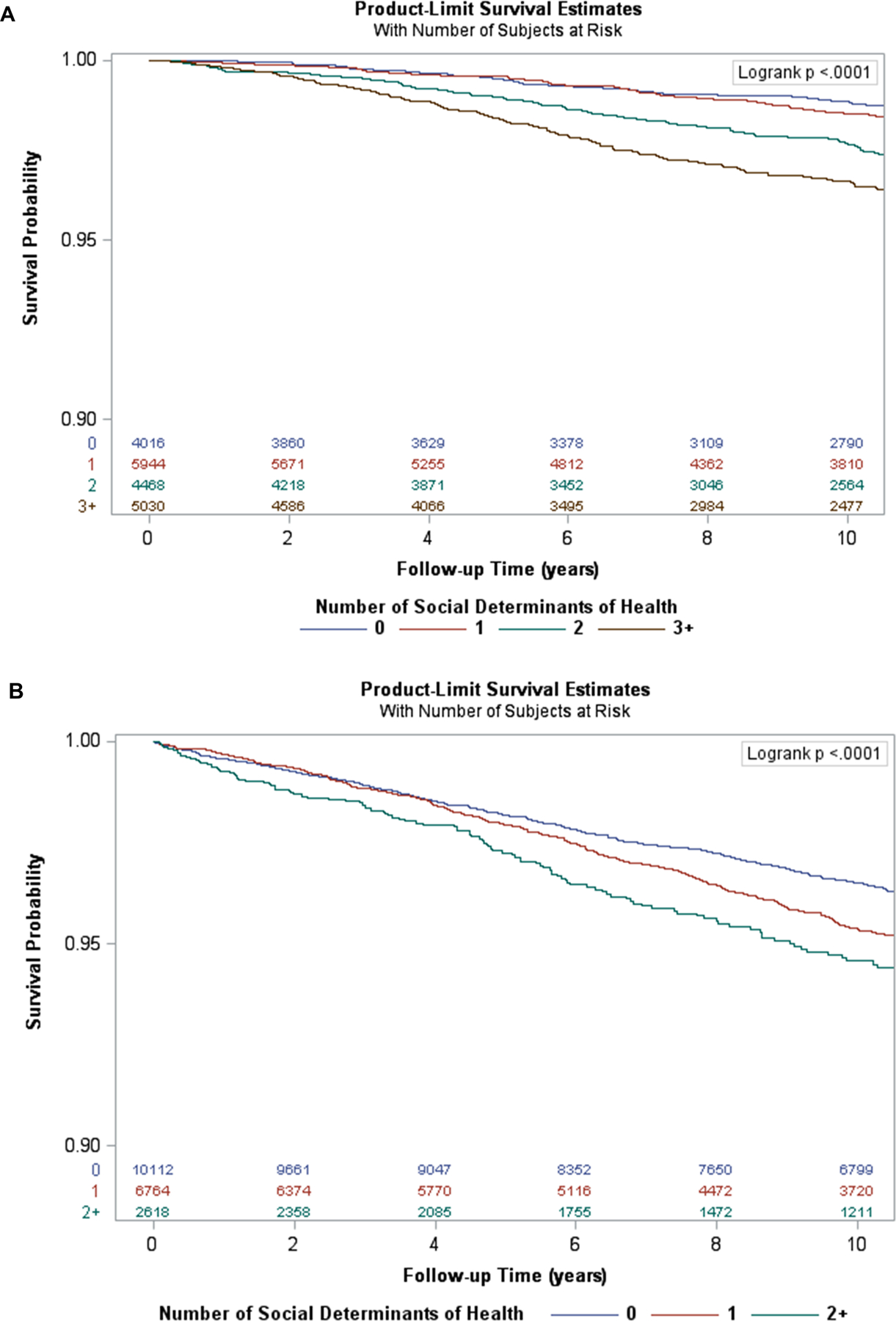
Results: Of 22 152 participants free of CHD at baseline, 58.8% were women and 42.0% were Black; 20.6% had no SDH, 30.6% had 1, 23.0% had 2, and 25.8% had ≥3. There were 463 fatal incident CHD events and 932 nonfatal MIs over a median of 10.7 years (interquartile range, 6.6 to 12.7). Fewer SDHs were associated with nonfatal MI than with fatal incident CHD. The age-adjusted incidence per 1000 person-years increased with the number of SDH for both fatal incident CHD (0 SDH, 1.30; 1 SDH, 1.44; 2 SDH, 2.05; ≥3 SDH, 2.86) and nonfatal MI (0 SDH, 3.91; 1 SDH, 4.33; ≥2 SDH, 5.44). Compared with those without SDH, crude and fully adjusted hazard ratios for fatal incident CHD among those with ≥3 SDH were 3.00 (95% CI, 2.17 to 4.15) and 1.67 (95% CI, 1.18 to 2.37), respectively; hazard ratios for nonfatal MI among those with ≥2 SDH were 1.57 (95% CI, 1.30 to 1.90) and 1.14 (95% CI, 0.93 to 1.41), respectively.
Conclusions: A greater burden of SDH was associated with a graded increase in risk of incident CHD, with greater magnitude and independent associations for fatal incident CHD. Counting the number of SDHs may be a promising approach that could be incorporated into clinical care to identify individuals at high risk of CHD.
Keywords: coronary disease; risk factors; social determinants of health.
Conflict of interest statement
Conflicts of Interest
MMS and PMM receive research grant funding from Amgen, Inc. None of the other authors have any conflicts of interest to report.
Figures
References
-
- AHRQ. National Healthcare Disparities Report 2003; http://www.qualitytools.ahrq.gov/disparitiesreport/download_report.aspx, 2003.
-
- AHRQ. 2015 National Healthcare Quality and Disparities Report and 5th Anniversary Update on the National Quality Strategy Rockville, MD: AHRQ; 2016.
-
- CDC. CDC Health Disparities and Inequalities Report - United States, 2013 Atlanta, GA: November 22 2013.
-
- Institute of Medicine. Guidance for the National Healthcare Disparities Report Washington, DC: National Academy Press; 2002. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
