

Effect of duration of adjuvant chemotherapy for patients with stage III colon cancer (IDEA collaboration): final results from a prospective, pooled analysis of six randomised, phase 3 trials
- PMID: 33271092
- PMCID: PMC7786835
- DOI: 10.1016/S1470-2045(20)30527-1
Effect of duration of adjuvant chemotherapy for patients with stage III colon cancer (IDEA collaboration): final results from a prospective, pooled analysis of six randomised, phase 3 trials
Abstract
Background: A prospective, pooled analysis of six randomised phase 3 trials was done to investigate disease-free survival regarding non-inferiority of 3 months versus 6 months of adjuvant chemotherapy for patients with stage III colon cancer; non-inferiority was not shown. Here, we report the final overall survival results.
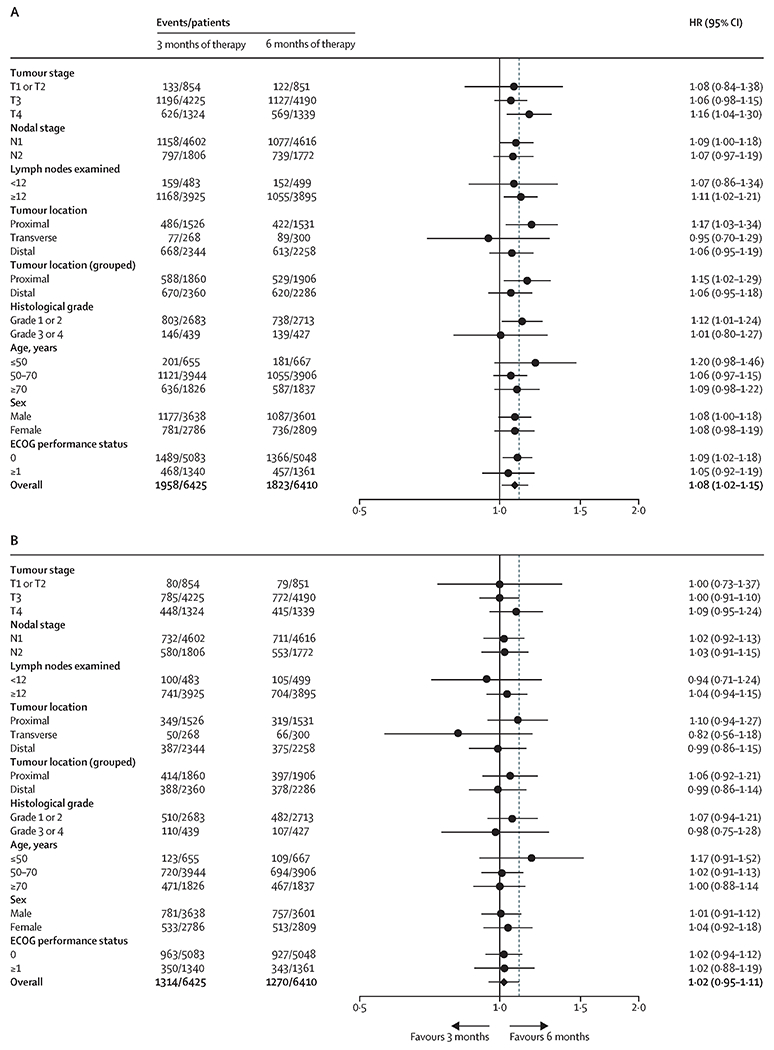
Methods: In this prospective, pooled analysis of six randomised phase 3 trials, we included patients with stage III colon cancer aged at least 18 years with an Eastern Cooperative Oncology Group performance status of 0-1 recruited between June 20, 2007, and Dec 31, 2015, across 12 countries in the CALGB/SWOG 80702, IDEA France, SCOT, ACHIEVE, TOSCA, and HORG trials, who started any treatment (modified intention-to-treat). Patients in all trials were randomly assigned to 3 months or 6 months of adjuvant fluorouracil, leucovorin, and oxaliplatin (FOLFOX) every 2 weeks or capecitabine and oxaliplatin (CAPOX) in different doses and methods every 3 weeks, at the treating physician's discretion. The primary endpoint was disease-free survival (time to relapse, secondary colorectal primary tumour, or death due to all causes), and overall survival (time to death due to all causes) was the prespecified secondary endpoint. The non-inferiority margin for overall survival was set as a hazard ratio (HR) of 1·11. Pre-planned subgroup analyses included regimen and risk group. Non-inferiority was declared if the one-sided false discovery rate adjusted (FDRadj) p value was less than 0·025.
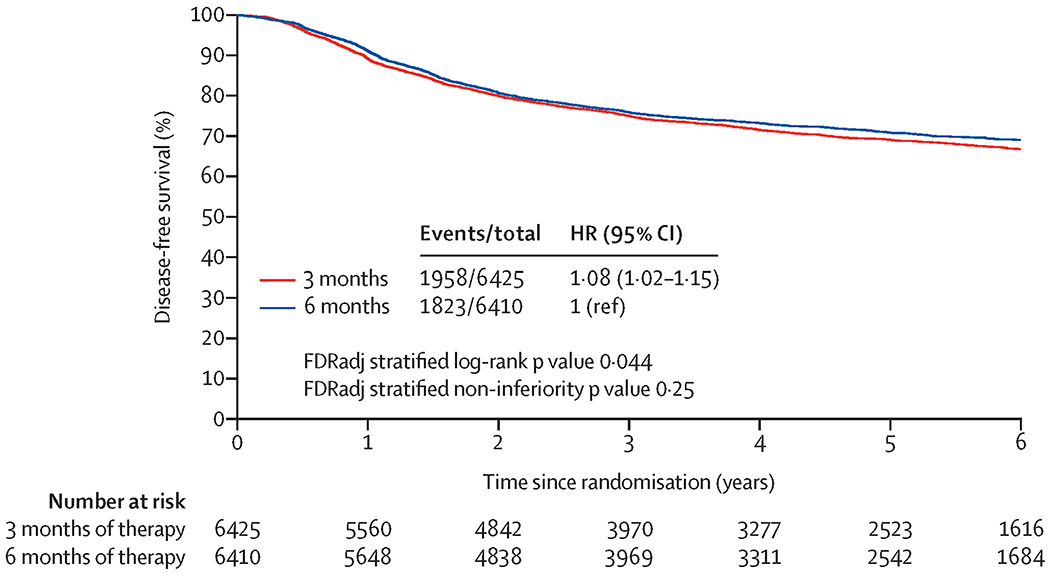
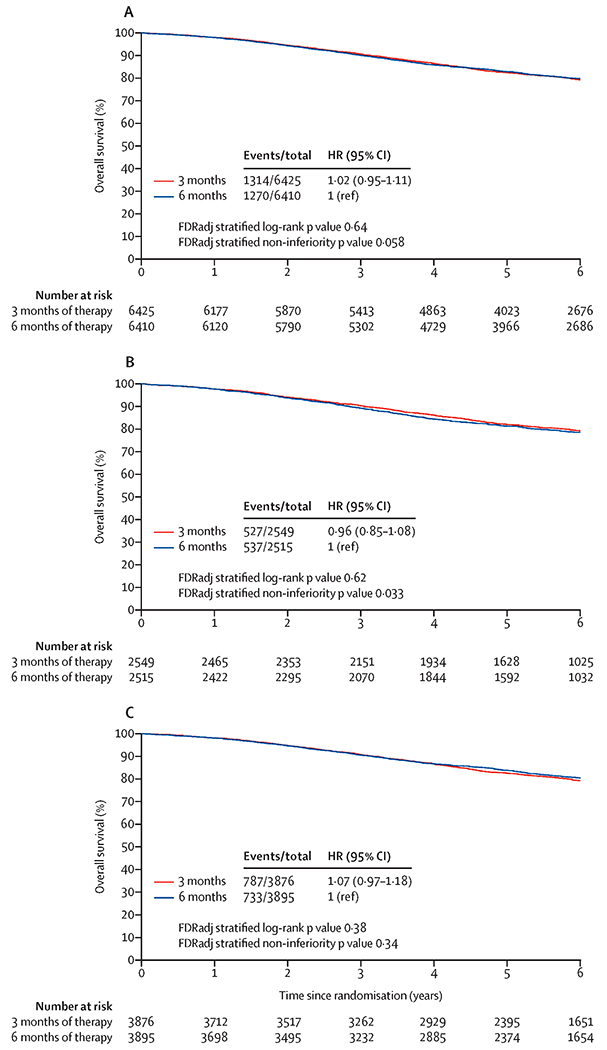
Findings: With median follow-up of 72·3 months (IQR 72·2-72·5), 2584 deaths among 12 835 patients were observed. 5064 (39·5%) patients received CAPOX and 7771 (60·5%) received FOLFOX. 5-year overall survival was 82·4% (95% CI 81·4-83·3) with 3 months of therapy and 82·8% (81·8-83·8) with 6 months of therapy (HR 1·02 [95% CI 0·95-1·11]; non-inferiority FDRadj p=0·058). For patients treated with CAPOX, 5-year overall survival was 82·1% (80·5-83·6) versus 81·2% (79·2-82·9; HR 0·96 [0·85-1·08]); non-inferiority FDRadj p=0·033), and for patients treated with FOLFOX 5-year overall survival was 82·6% (81·3-83·8) and 83·8% (82·6-85·0; HR 1·07 [0·97-1·18]; non-inferiority FDRadj p=0·34). Updated disease-free survival results confirmed previous findings (HR 1·08 [95% CI 1·02-1·15]; non-inferiority FDRadj p=0·25). Data on adverse events were not further recorded.
Interpretation: Non-inferiority of 3 months versus 6 months of adjuvant chemotherapy for patients with stage III colon cancer was not confirmed in terms of overall survival, but the absolute 0·4% difference in 5-year overall survival should be placed in clinical context. Overall survival results support the use of 3 months of adjuvant CAPOX for most patients with stage III colon cancer. This conclusion is strengthened by the substantial reduction of toxicities, inconveniencies, and cost associated with a shorter treatment duration.
Funding: US National Cancer Institute.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Duration of adjuvant treatment for patients with stage III colon cancer.Lancet Oncol. 2020 Dec;21(12):1545-1547. doi: 10.1016/S1470-2045(20)30618-5. Lancet Oncol. 2020. PMID: 33271085 No abstract available.
References
-
- Moertel CG, Fleming TR, Macdonald JS, et al. Levamisole and fluorouracil for adjuvant therapy of resected colon carcinoma. N Engl J Med 1990; 322(6): 352–8. - PubMed
-
- Haller DG, Catalano PJ, Macdonald JS, et al. Phase III study of fluorouracil, leucovorin, and levamisole in high-risk stage II and III colon cancer: final report of Intergroup 0089. J Clin Oncol 2005; 23(34): 8671–8. - PubMed
-
- Sargent DJ, Wieand HS, Haller DG, et al. Disease-free survival versus overall survival as a primary end point for adjuvant colon cancer studies: individual patient data from 20,898 patients on 18 randomized trials. J Clin Oncol 2005; 23(34): 8664–70. - PubMed
-
- Andre T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med 2004; 350(23): 2343–51. - PubMed
-
- Haller DG, Tabernero J, Maroun J, et al. Capecitabine plus oxaliplatin compared with fluorouracil and folinic acid as adjuvant therapy for stage III colon cancer. J Clin Oncol 2011; 29(11): 1465–71. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
