

A Randomized Trial Evaluating Online 3-Dimensional Optical Frequency Domain Imaging-Guided Percutaneous Coronary Intervention in Bifurcation Lesions
- PMID: 33272034
- PMCID: PMC7732152
- DOI: 10.1161/CIRCINTERVENTIONS.120.009183
A Randomized Trial Evaluating Online 3-Dimensional Optical Frequency Domain Imaging-Guided Percutaneous Coronary Intervention in Bifurcation Lesions
Abstract
Background: Clinical implications of online 3-dimensional optical frequency domain imaging (3D-OFDI)-guided stenting for bifurcation lesions have not been investigated in the randomized controlled trials. The purpose of this study was to determine whether online 3D-OFDI-guided stenting is superior to angiography-guided percutaneous coronary intervention (PCI) in terms of incomplete stent apposition at the bifurcation segment.
Methods: The OPTIMUM trial (Online 3-Dimensional Optical Frequency Domain Imaging to Optimize Bifurcation Stenting Using UltiMaster Stent) was a randomized, multicenter clinical trial. Eligible patients had an angiographically significant stenosis in the bifurcation lesion treated with a provisional single stent strategy using the Ultimaster sirolimus eluting stent. Patients were randomly allocated to either online 3D-OFDI-guided or angiography-guided PCI. Patients randomized to 3D-OFDI guidance underwent online 3D-OFDI assessment after rewiring into the jailed side branch after stenting and proximal optimization technique, while in the angiography guidance arm, rewiring was performed using conventional fluoroscopic/angiographic guidance. The primary end point of this trial was the postprocedural average percentage of malapposed struts per lesion assessed by OFDI in the confluence zone of the main and side branches.
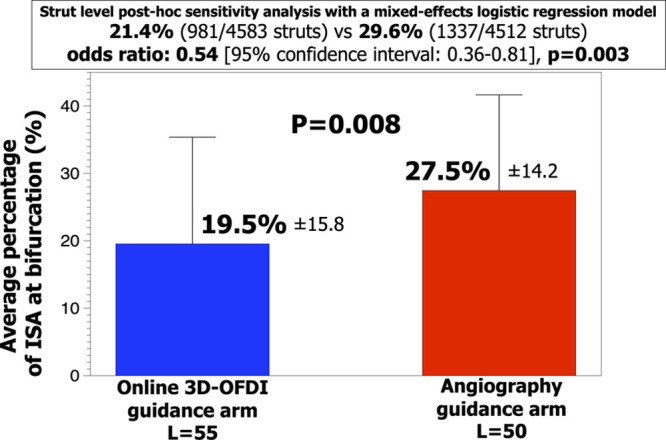
Results: Between June 8, 2017 and September 26, 2018, 110 patients with 111 bifurcation lesions were randomized at 4 Japanese centers. Of these, 56 patients with 57 lesions were treated with 3D-OFDI-guided PCI, whereas 54 patients with 54 lesions were treated with angiography-guided PCI. In the 3D-OFDI guidance arm, the feasibility of online 3D-OFDI was 98.2%. The average percentage of incomplete stent apposition per lesion at bifurcation was lower in the 3D-OFDI guidance arm than that in the angiography guidance arm (19.5±15.8% versus 27.5±14.2%, P=0.008). The superiority of the 3D-OFDI guidance arm was also confirmed in the strut level analysis (odds ratio: 0.54 [95% CI, 0.36-0.81]; P=0.003).
Conclusions: Online 3D-OFDI-guided bifurcation PCI was superior to angiography-guided bifurcation PCI in terms of acute incomplete stent apposition at bifurcation. Registration: URL: https://www.clinicaltrials.gov. Unique identifier: NCT02972489.
Keywords: angiography; dilatation; odds ratio; percutaneous coronary intervention; stent.
Conflict of interest statement
Dr Sotomi reports personal fees from Terumo Corporation, during the conduct of the study; personal fees from Bayer, personal fees from Daiichi-Sankyo, personal fees from Amgen Astellas BioPharma, personal fees from Boehringer Ingelheim, personal fees from Bristole-Myers Squibb, personal fees from Abbott Vascular Japan, personal fees from Boston Scientific Japan, personal fees from Cardinal Health, personal fees from Medtronic, personal fees from Biosensors, outside the submitted work. Dr Muramatsu reports research grants to Fujita Health University from Terumo Corporation, Tokyo, Japan. Dr Ozaki reports research grants to Fujita Health University from Terumo Corporation, Tokyo, Japan. Dr Serruys reports personal fees from Abbott Laboratories, AstraZeneca, Biotronik, GLG Research, Medtronic, Sino Medical Sciences Technology, Société Europa Digital Publishing, Stentys France, Svelte Medical Systems, Philips/Volcano, St Jude Medical, Qualimed, and Xeltis, outside the submitted work. Dr Okamura reports personal fees from Terumo Corporation, during the conduct of the study; personal fees from Abbot Vascular Japan, personal fees from Medtronic, personal fees from Edwards Life Science, personal fees from Boston Scientific Japan, personal fees from Daiichi Sankyo, personal fees from Astellas, personal fees from Boehringer Ingelheim, personal fees from MSD, personal fees from Sanofi, personal fees from Tanabe Mitsubishi, outside the submitted work. The other authors report no conflicts.
Figures


References
-
- Lassen JF, Holm NR, Stankovic G, Lefèvre T, Chieffo A, Hildick-Smith D, Pan M, Darremont O, Albiero R, Ferenc M, et al. Percutaneous coronary intervention for coronary bifurcation disease: consensus from the first 10 years of the European bifurcation club meetings. EuroIntervention. 2014;10:545–560. doi: 10.4244/EIJV10I5A97 - PubMed
-
- Asakura T, Karino T. Flow patterns and spatial distribution of atherosclerotic lesions in human coronary arteries. Circ Res. 1990;66:1045–1066. doi: 10.1161/01.res.66.4.1045 - PubMed
-
- Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet JP, Falk V, Head SJ, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165. doi: 10.1093/eurheartj/ehy394 - PubMed
-
- Banning AP, Lassen JF, Burzotta F, Lefèvre T, Darremont O, Hildick-Smith D, Louvard Y, Stankovic G. Percutaneous coronary intervention for obstructive bifurcation lesions: the 14th consensus document from the European bifurcation club. EuroIntervention. 2019;15:90–98. doi: 10.4244/EIJ-D-19-00144 - PubMed
-
- Onuma Y, Katagiri Y, Burzotta F, Holm NR, Amabile N, Okamura T, Mintz GS, Darremont O, Lassen JF, Lefèvre T, et al. Joint consensus on the use of OCT in coronary bifurcation lesions by the European and Japanese bifurcation clubs. EuroIntervention. 2019;14:e1568–e1577. doi: 10.4244/EIJ-D-18-00391 - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
