

Safety and clinical efficacy of BCMA CAR-T-cell therapy in multiple myeloma
- PMID: 33272302
- PMCID: PMC7713173
- DOI: 10.1186/s13045-020-01001-1
Safety and clinical efficacy of BCMA CAR-T-cell therapy in multiple myeloma
Abstract
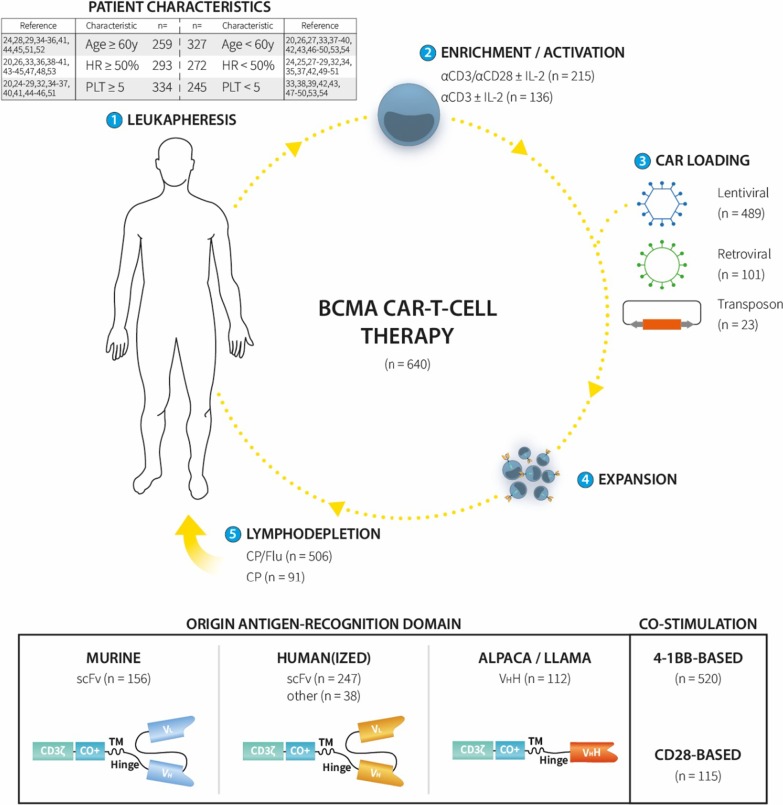
Background: B-cell maturation antigen (BCMA)-targeted chimeric antigen receptor (CAR)-T-cell therapy is an emerging treatment option for multiple myeloma. The aim of this systematic review and meta-analysis was to determine its safety and clinical activity and to identify factors influencing these outcomes.
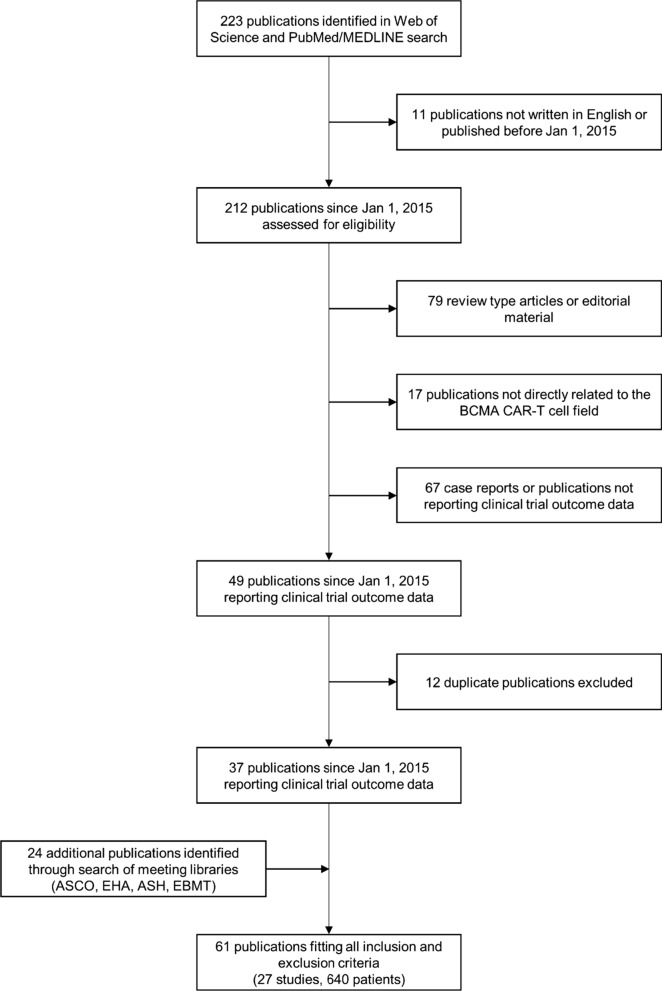
Methods: We performed a database search using the terms "BCMA," "CAR," and "multiple myeloma" for clinical studies published between 01/01/2015 and 01/01/2020. The methodology is further detailed in PROSPERO (CRD42020125332).
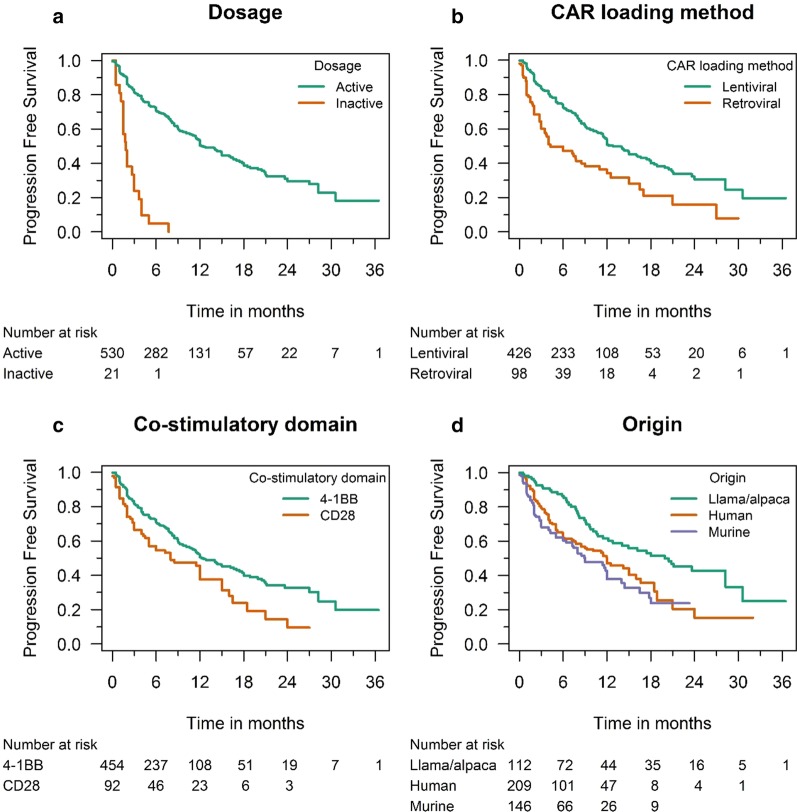
Results: Twenty-three different CAR-T-cell products have been used so far in 640 patients. Cytokine release syndrome was observed in 80.3% (69.0-88.2); 10.5% (6.8-16.0) had neurotoxicity. A higher neurotoxicity rate was reported in studies that included more heavily pretreated patients: 19.1% (13.3-26.7; I2 = 45%) versus 2.8% (1.3-6.1; I2 = 0%) (p < 0.0001). The pooled overall response rate was 80.5% (73.5-85.9); complete responses (CR) were observed in 44.8% (35.3-54.6). A pooled CR rate of 71.9% (62.8-79.6; I2 = 0%) was noted in studies using alpaca/llama-based constructs, whereas it was only 18.0% (6.5-41.1; I2 = 67%) in studies that used retroviral vectors for CAR transduction. Median progression-free survival (PFS) was 12.2 (11.4-17.4) months, which compared favorably to the expected PFS of 1.9 (1.5-3.7) months (HR 0.14; p < 0.0001).
Conclusions: Although considerable toxicity was observed, BCMA-targeted CAR-T-cell therapy is highly efficacious even in advanced multiple myeloma. Subgroup analysis confirmed the anticipated inter-study heterogeneity and identified potential factors contributing to safety and efficacy. The results of this meta-analysis may assist the future design of CAR-T-cell studies and lead to optimized BCMA CAR-T-cell products.
Keywords: BCMA; CAR-T; Multiple myeloma.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
